HIPAA by itself no longer covers the job. If I run privacy or compliance in healthcare, I now have to track federal rules, state health-data laws, vendor risk, and new AI duties at the same time.
Here’s the short version:
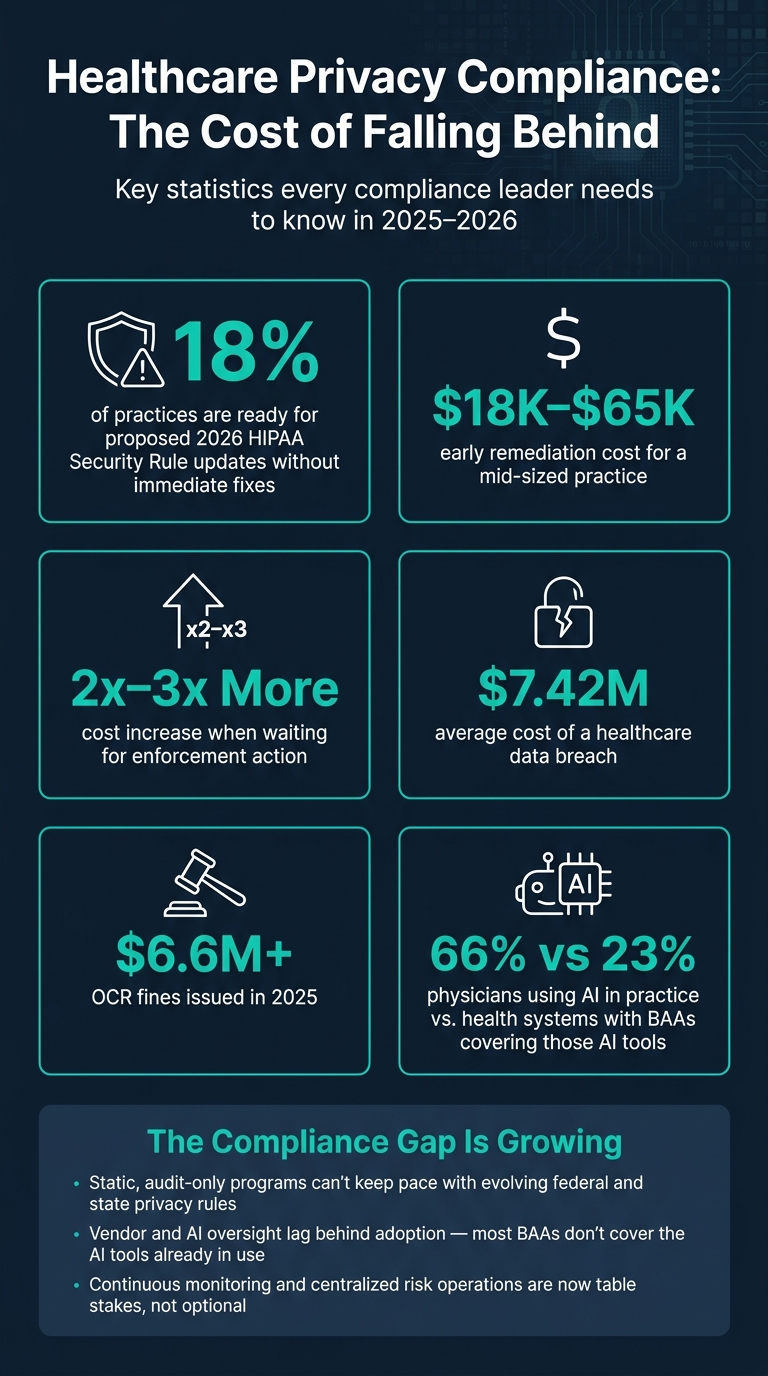
- Static compliance programs are falling behind.
- Only 18% of practices are ready for the proposed 2026 HIPAA Security Rule updates without immediate fixes.
- Fixing gaps early can cost $18,000 to $65,000 for a mid-sized practice.
- Waiting for enforcement can push costs to 2x to 3x more.
- The average healthcare breach cost is about $7.42 million.
- In 2025, OCR fines topped $6.6 million.
- 66% of U.S. physicians were already using AI in clinical practice by early 2026, but only 23% of health systems had BAAs that covered those AI tools.
So what should I do?
I’d keep the program simple and risk-based:
- Put privacy, security, legal, IT, and clinical teams under one governance group
- Map laws to one shared set of controls
- Keep a live inventory of PHI, systems, devices, and vendors
- Classify data so tighter controls go to higher-risk systems
- Tier vendors by risk and follow a guide to HIPAA-compliant vendor risk management to reassess high-risk ones on a set schedule
- Keep audit evidence ready at all times, not just before a review
- Use automation for repeat tasks, but keep people in charge of final decisions
The article’s main point is clear: privacy readiness now depends on clear ownership, live data visibility, vendor review, and timestamped evidence. That shift moves a healthcare team from audit prep to day-to-day control.
Healthcare Privacy Compliance: The Cost of Falling Behind in 2025–2026
HIPAA Compliance for Healthcare IT
sbb-itb-535baee
The Compliance Gaps Healthcare Organizations Need to Close
Healthcare organizations are running into three clear operational gaps: fragmented controls, limited data visibility, and manual audit evidence. The first problem is control fragmentation.
Fragmented Rules and Inconsistent Control Mapping
In many multi-law programs, privacy, security, and AI controls end up in separate workflows. On paper, that can look organized. In practice, it often means duplicated work, mixed interpretations, and controls that seem aligned but aren't.
One common breakdown happens when privacy and security teams split ownership. Privacy teams usually manage consumer requests and marketing cookies. Security teams usually manage HIPAA and technical safeguards. When those groups work in separate tracks and report through different chains, the same PHI can end up under two different control sets without anyone tying it together [1].
HIPAA also has limits. It does not cover consumer-rights duties such as access, purpose limitation, or opt-out requirements.
Once PHI is reused for marketing or analytics, HIPAA no longer sets the full privacy standard. State laws do [1].
Limited Visibility Into PHI, Systems, and Vendors
PHI moves through EHRs, cloud apps, devices, and vendors. But many organizations still manage ownership in spreadsheets. That's a problem. It becomes hard to keep a complete, current view of where data lives and who owns it [2].
The vendor blind spot is hard to ignore. Only 23% of health systems have BAAs that cover the specific AI tools their physicians use, even though 66% of U.S. physicians were already using AI in clinical practice as of early 2026 [3]. Put simply, adoption moved faster than vendor oversight. And regulators don't give the primary organization a pass just because a third party caused the issue. If a vendor fails a control, it becomes your audit problem [2].
New AI governance rules add another weak spot when oversight and bias monitoring are not documented [2]. Downstream vendors bring added risk that most inventories still miss.
When ownership isn't clear, audit evidence starts to fall apart.
How Static Compliance Workflows Create Audit Risk
Point-in-time assessments leave room for gaps between reviews, especially when regulators ask for operational evidence [2].
The same failure patterns show up again and again:
- Missing timestamps
- Inconsistent execution records
- Outdated policy approvals [2]
These issues tend to surface when compliance runs on manual workflows instead of continuous monitoring and controls validation.
"Evidence is what regulators examine, not intent." - Zoya Khan, Product Management and Operations, VComply [2]
Static programs review controls at one moment in time. Adaptive frameworks monitor evidence on a continuing basis and reuse it across requirements. That difference matters. Manual workflows can lead straight to failed audits, missing evidence, and enforcement exposure.
The financial pressure is already there. OCR fined more than $6.6 million in 2025, and the average healthcare breach cost was about $7.42 million [2][3]. Closing these gaps means using one operating model for governance, data visibility, vendor oversight, and monitoring.
A Practical Framework for Meeting New Privacy Requirements
Fixing the gaps above takes more than patching one control at a time. It takes a clear model that can work across current laws and whatever comes next. If governance sits in one lane, inventory in another, and monitoring somewhere else, teams end up with gaps, overlap, and messy audits. The framework below is built on three working pillars: governance and regulatory mapping, data inventory and risk assessment, and third-party controls with continuous monitoring.
Governance, Scope, and Regulatory Mapping
Start with accountability. Set up a formally chartered privacy and security governance committee with leaders from compliance, legal, privacy, security, IT, clinical operations, and key business units. This group approves policies, reviews risk reports, sets remediation priorities, and reports up to executive leadership.
Next comes scope. The program should cover every business unit that handles PHI or sensitive health-related data. That includes clinical operations, revenue cycle, telehealth, and research, plus every system, data store, and vendor that stores, processes, or transmits that data.
Then build a current regulatory tracker. It should list every rule that applies, including HIPAA/HITECH, 42 CFR Part 2, state breach notification laws, California's CPRA, and Washington's My Health My Data Act. Review the tracker at least quarterly. When a new rule shows up, it should trigger a review of the control areas it affects, not force a full rebuild of the program.
The big time-saver comes from mapping those rules to a shared control library. One well-built access control or encryption standard can meet requirements across several laws at the same time. Here’s what that looks like in practice:
| Requirement Source | Requirement Focus | Common Control | Sample Control Activity |
|---|---|---|---|
| HIPAA Security Rule (45 CFR 164.312) | Technical safeguards for ePHI | Access Control | Enforce role-based access and MFA for all PHI systems |
| HIPAA Security Rule (45 CFR 164.312(c)) | Integrity and protection of ePHI | Logging & Monitoring | Enable audit logs for PHI access, changes, and exports; review high-risk events weekly |
| HIPAA Privacy Rule (45 CFR 164.530(b)) | Workforce training | Training & Awareness | Require initial and annual privacy/security training with completion tracking |
| HIPAA Privacy Rule (45 CFR 164.530(c)) | Safeguards to protect PHI | Encryption | Encrypt PHI at rest and in transit using TLS 1.2+ |
| State consumer privacy law | Consumer rights (access, deletion) | Data Governance & Retention | Build data subject request workflows; define retention schedules and secure deletion |
Data Inventory, Classification, and Risk Assessment
Once ownership is set, the next job is getting a live picture of what the program actually covers. Build one inventory for every application, database, medical device, and vendor that touches PHI or PII. For each item, record the data type, data subjects, hosting model, integrations, and location.
That inventory works best when paired with a simple classification model:
- Restricted: PHI, full medical records, SSNs
- Confidential: health-adjacent identifiable data, non-public employee information
- Internal
- Public
Classification should drive safeguards. Restricted systems need tighter access controls, more frequent log reviews, and stricter retention rules.
Risk assessments should follow that same logic. PHI-heavy systems should get annual enterprise-level assessments at a minimum, with extra reviews triggered by major IT deployments, mergers, or new telehealth platforms. Each assessment should look at threats such as ransomware, insider misuse, cloud misconfigurations, and third-party failures. It should also feed a risk register that ranks findings by patient privacy impact, regulatory exposure, and operational disruption. That ranking gives leadership a practical way to decide where remediation dollars and staff time should go first.
Third-Party Controls, Policy Updates, and Continuous Monitoring
After mapping PHI and internal systems, apply the same discipline to vendors and downstream tools. Vendor risk does not stop when the contract is signed. Every vendor with PHI access should get a risk tier based on the sensitivity of the data involved and how critical the service is. High-tier vendors, such as EHR platforms, cloud infrastructure providers, and telehealth systems, need full due diligence, executed BAAs, and scheduled reassessments.
Policy updates and staff training should connect directly to the regulatory tracker. When a new law takes effect or OCR issues updated guidance, the affected policies should be flagged for revision, and training should be updated with them. Privacy impact reviews should also be part of intake for any new technology, including AI tools, so teams assess risk before deployment instead of cleaning up problems later.
The framework should keep producing audit artifacts as part of normal operations: access logs, training completion records, vendor assessment results, and policy approval timestamps. Automation can help generate evidence on a continuous basis, but people should still review and approve final decisions. Censinet RiskOps™ can support that model by centralizing risk assessments, automating workflows, and preserving oversight. Automation can generate evidence continuously, with human review reserved for exceptions.
Putting the Framework Into Practice With Technology and Automation
Centralized Risk Operations for Healthcare
A framework only works if teams can use it every day. If vendor questionnaires are buried in email, risk findings live in spreadsheets, and audit evidence is scattered across shared drives, progress slows down. Gaps in documentation start to pile up, and that can draw scrutiny from OCR or state attorneys general. At that point, the framework stops being a working system and turns into a paper policy no one can run from.
For healthcare teams, one system should tie together assessments, remediation, and evidence. A centralized platform can do that by bringing controls, assessments, remediation tasks, vendor questionnaires, and audit evidence into a single system of record, all tied to one control library and regulatory map. Privacy, security, compliance, and supply chain teams can then work from the same view of open risks and pending tasks, with workflows that assign owners and track due dates automatically.
That setup also makes audit prep much less painful. BAAs, SOC 2 reports, and policy documents can be linked to the right vendor, system, or control, so teams can pull what they need fast. If a new cloud-based patient engagement tool needs review, supply chain can kick off a standard assessment directly in the platform. The vendor gets a tailored questionnaire mapped to HIPAA safeguards and any state law that applies. Responses are scored automatically, and gaps go to the right reviewers.
The same model helps with medical devices. Clinical engineering can keep a live inventory, score medical device security risks, and trigger remediation when support ends or a serious vulnerability appears. Censinet RiskOps™ supports this model across PHI, clinical applications, medical devices, and supply chains.
Automation and AI With Human Oversight
Once workflows are centralized, automation can take a lot of the manual drag out of the process. It works best on tasks that are structured, repetitive, and time-consuming. That includes routing new vendor intake forms based on data sensitivity, sending reminders for overdue assessments, and pulling standard evidence from a central repository. NIST guidance notes that automation works best when it handles well-defined, repeatable work, which leaves people free to spend time on judgment calls that are harder to standardize.[4] The point isn't just speed. Automation should also create traceable evidence.
Final risk decisions should still stay with people. Censinet AI™ pushes this further by speeding up the assessment process itself. It helps vendors complete security questionnaires faster, summarizes vendor evidence and documentation automatically, captures downstream vendor risks, and drafts summary reports using the full set of assessment data.
Censinet AI uses a human-in-the-loop model. Risk teams keep control through configurable rules and review processes, so the system supports decision-making instead of taking it over. The same workflow can send AI-related findings to designated reviewers and pull them into one risk dashboard.
Conclusion: Moving From Reactive Compliance to Continuous Privacy Readiness
The core issue hasn’t changed: privacy rules shift, data flows change, and vendor risk never sits still. What has changed is the price of falling behind. Healthcare data breaches now average $7.42 million per incident [2], and an audit-only approach just doesn’t hold up in that kind of setting.
That’s why the framework matters. It brings control mapping into one place, keeps inventories up to date, and connects remediation to ongoing monitoring. In plain English, it tackles the fragmented rules, poor visibility, and manual workflows covered earlier. The result is a program that stays audit-ready between reviews, not only when an audit is on the calendar.
Continuous readiness also depends on clear ownership, timestamped and version-controlled evidence, and closed-loop remediation with documented corrective actions and retesting.
Censinet RiskOps™ can support this model by centralizing PHI risk, managing third-party risk, medical-device risk, and AI governance. The aim is continuous privacy readiness, not point-in-time compliance.
FAQs
What counts as a live compliance program?
A live compliance program works like a connected, continuous system, not a static document or a once-a-year checklist. Its parts need to function day to day, be documented, and be measured by actual results.
It also moves compliance from reactive, periodic checks to proactive, real-time oversight that spots, tracks, and addresses risks as they come up. Tools like Censinet RiskOps™ can help automate these workflows and keep them aligned with changing regulatory frameworks.
Which vendors should we reassess first?
Start by sorting vendors into risk tiers, and put high-risk vendors at the top of the list.
Focus first on vendors that:
- have direct access to protected health information
- support core clinical systems
- serve as a single point of failure
That usually includes vendors like EHR providers, medical device manufacturers, and cloud-based data storage services.
You should also move vendors that handle substance use disorder data to the front of the line so you can meet specific regulatory deadlines.
Censinet RiskOps™ can help you keep your vendor inventory accurate and flag high-risk business associates.
How can we use AI without creating compliance risk?
Use a governance framework from day one. Get a Business Associate Agreement (BAA) in place before you handle PHI. Skip consumer-grade AI tools if they don't offer one. And follow the minimum necessary standard, which means sharing only the data needed for the task at hand.
Platforms like Censinet RiskOps™ can help automate third-party risk assessments, keep audit trails in order, and support continuous monitoring of AI systems.
