Most community clinics do not need a big AI program. They need a small set of rules they can use now. With more than 100 million Americans facing primary care access issues, and fewer than 60% of organizations having finished a formal AI risk review, I see the gap clearly: AI is already in care, but oversight often is not.
Here’s the short version:
- Large health system governance does not fit small clinics well. Community providers often have lean teams, tight budgets, and heavy reliance on vendor tools.
- The legal and safety risks stay the same. HIPAA, state privacy rules, cyber risk, and patient safety duties still apply.
- Most AI in community care comes from vendors. That means oversight should focus on procurement, contracts, BAAs, data use, and model changes.
- A usable model is small and tied to daily work. I’d keep it to a small cross-functional group, a basic AI inventory, simple risk tiers, and clear human review rules.
- High-risk uses need closer review. That includes triage, diagnostic support, patient-facing recommendations, and anything that affects the medical record or coverage decisions.
- Small teams can extend current workflows instead of building a new program. Add a short review of third-party AI risk to vendor intake, HIPAA risk review, and incident reporting.
- Day-to-day controls matter most. Least-privilege access, short data flow maps, retention limits, staff training, consent for recording where state law requires it, and clear suspension rules all help keep use in check.
A simple way to think about it: if AI is part of scheduling, notes, triage, billing, or patient calls, it needs plain rules that staff can follow on a busy day.
| Area | What community providers need |
|---|---|
| Governance team | Small group with named decision-makers |
| AI tracking | Basic inventory of tools, data, owners, and review dates |
| Risk review | Short AI add-on in current vendor and privacy workflows |
| Human oversight | Required for clinical, record, eligibility, and patient-facing outputs |
| Vendor control | Contract terms on PHI, retention, training use, subprocessors, and breach notice |
| Daily use | Access limits, staff training, incident reporting, and stop-use triggers |
If I had to sum up the article in one line, it would be this: community healthcare needs AI governance that is lean, clear, and built for the way clinics already work.
Healthcare AI Governance - Risks, Compliance, and Frameworks Explained
sbb-itb-535baee
Why large-system AI governance does not work for community healthcare
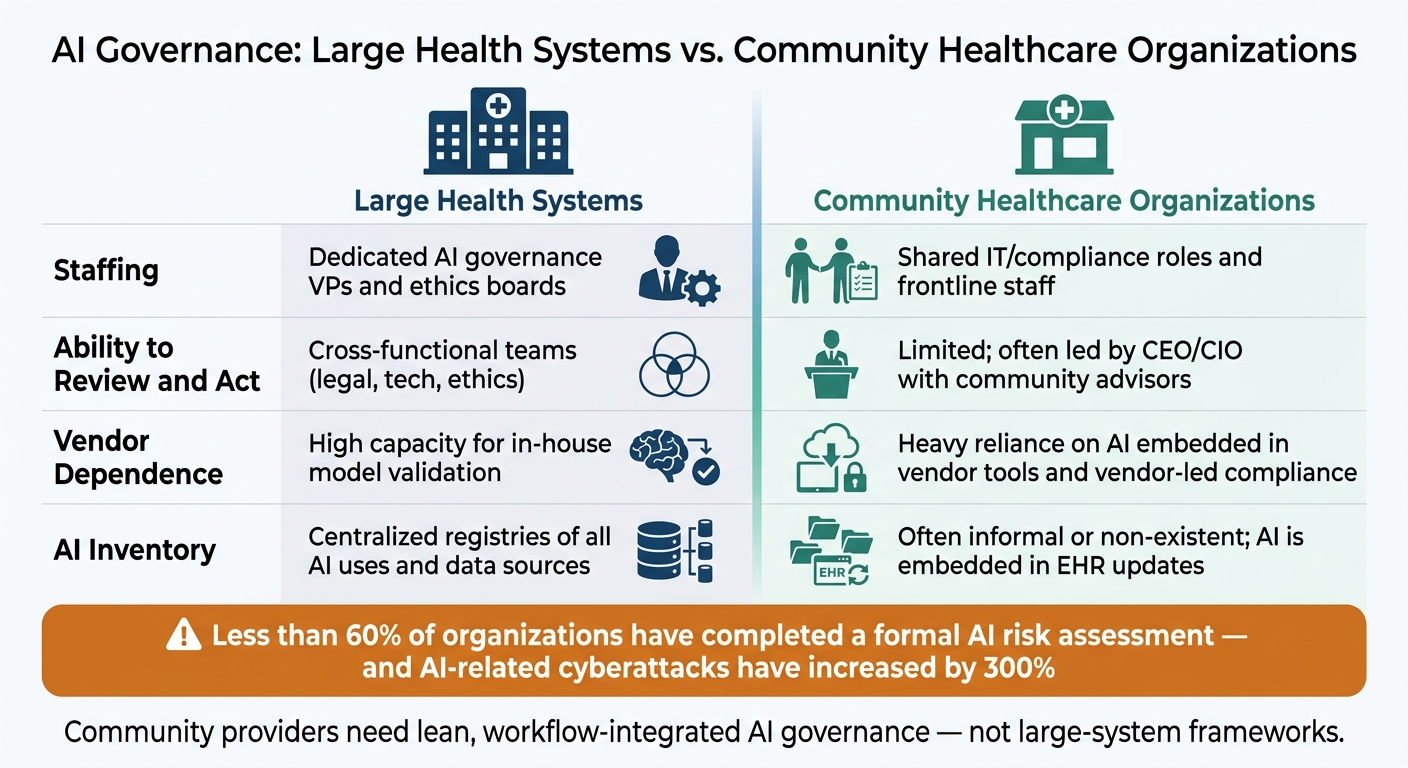
AI Governance: Large Health Systems vs. Community Healthcare Organizations
Large health systems can pay for dedicated AI governance teams and automated monitoring. Community providers usually can't. And that gap shows up fast in staffing, vendor review, and day-to-day monitoring.
This isn't only a matter of size. It's about whether governance can happen at all during normal clinic operations.
| Feature | Large Academic/Health Systems | Community Healthcare Organizations |
|---|---|---|
| Staffing | Dedicated AI governance VPs and ethics boards | Shared IT/compliance roles and frontline staff |
| Ability to Review and Act | Cross-functional teams (legal, tech, ethics) | Limited; often led by CEO/CIO with community advisors |
| Vendor Dependence | High capacity for in-house model validation | Heavy reliance on AI embedded in vendor tools and vendor-led compliance |
| AI Inventory | Centralized registries of all AI uses and data sources | Often informal or non-existent; AI is embedded in EHR updates |
Limited staff, budget, and capacity
In many clinics, one person is handling security, vendor management, reporting, and support. Adding a formal AI governance layer means adding one more job on top of patient care and core operations. That cost is real.
Each new review step, documentation task, or committee meeting takes time that staff don't have. On paper, a formal process can look reasonable. In practice, it can be too much for a small team trying to keep the doors open and care moving.
Heavy dependence on vendors and embedded AI
In community care, AI governance usually begins with the vendors already in the workflow. AI often shows up through product updates, not internal buildouts. That means changes can slip in with little or no notice.
A scheduling tool might quietly add an AI-driven prioritization layer. A documentation platform might update its ambient scribing model. If no one sees the change, no one reviews the risk. That's the problem in plain terms.
So in community care, AI governance is mostly a vendor oversight issue, not an internal model oversight issue.
The result: real risk without a workable control structure
Once AI is built into everyday tools, gaps start to open unless governance stays simple and tied to daily work. AI-related cyberattacks have recently increased by 300%, and less than 60% of organizations have completed formal AI risk assessments [1]. For community providers without dedicated oversight, that isn't just a data point. It's a live gap in cybersecurity, patient safety, and regulatory compliance.
Without an inventory, a vendor review process, and clear human-review rules, AI risk can grow quietly across cyber, safety, and compliance workflows. That's why the governance model needs to be small, visible, and part of daily operations.
What a right-sized AI governance model looks like in practice
Once the governance gap is clear, the next step is building a model people will actually use. The best setup is small, fast, and connected to day-to-day work. In plain English: fewer layers, clear ownership, and controls that fit what staff are doing every day.
A small cross-functional governance group with clear authority
Community healthcare organizations need a small cross-functional group that can make actual decisions, not just talk about them. That group should include clinical leadership, a compliance or privacy lead, someone from IT or cybersecurity, an operations representative, and a finance voice. Then assign clear roles: one owner for approvals, one for incidents, one for policy, and one for escalation.
For FQHCs and health centers, adding a community advisor can help flag language-access issues and local trust concerns that a technical team might miss.
A simple AI inventory and risk-tiering model
A governance group can't govern what it can't see. So the first job is a basic inventory. Before the group can act, it needs a working view of what AI is already being used in daily workflows. That starts with a list of each tool's purpose, data, and restrictions, along with the owner, data, risk tier, and review cadence for each one.
Once that inventory is in place, risk-tiering gets much easier:
| Risk Level | AI Tool Examples | Required Controls | Monitoring Frequency |
|---|---|---|---|
| High | Clinical triage, diagnostic aids, patient-facing recommendations | Mandatory human review, bias auditing, strict HIPAA encryption | Quarterly or real-time |
| Moderate | Ambient scribing, multilingual phone agents, insurance eligibility | Periodic spot checks of documentation, data-use audits, vendor risk assessment | Twice a year |
| Lower | Administrative drafting, appointment scheduling, internal workflow automation | Initial vendor security review, staff training on privacy, incident reporting | Annually |
This kind of tiering keeps the workload under control. High-risk tools get close attention. Lower-risk tools get a lighter touch. The inventory should also be updated when AI use cases, data, or controls change.
Human review rules that match the level of risk
After inventory comes control: decide which outputs need human sign-off and which do not. Not every AI output needs a clinician review before it moves forward. But some clearly do. The point is to spell this out, so staff don't have to guess.
Human review should be required when AI outputs affect clinical triage, are entered into the medical record, affect eligibility or coverage decisions, or are shown to patients as recommendations. State rules already point toward mandatory human review for clinical AI and no AI-only coverage denials. Even where state law does not yet require it, these are sensible defaults for patient safety and record integrity.
For lower-risk tools like administrative drafting, internal scheduling automation, and revenue cycle workflows, a final human review before outputs go external is usually enough. Those tools can move with light review and routine reporting.
How to assess AI risk and manage vendors without overwhelming small teams
Once your human-review rules are in place, the next step is simple: use an assessment process that a small team can actually run.
Most small teams do not need a separate AI governance program. A better move is to extend the workflows you already have for HIPAA risk analysis, vendor intake, and BAA review with a short AI supplement.
Right-sized assessments for clinical and administrative AI
The HHS Security Rule already requires an "accurate and thorough assessment of potential risks and vulnerabilities to ePHI" as part of the security program.[5] That same duty applies when an AI tool touches patient data.
So instead of spinning up a brand-new review process, add a short AI section to your current vendor due-diligence packet.
The main questions are pretty direct:
- Does the system create, access, store, or transmit PHI?
- Can data be kept or reused to train models?
- Are outputs used in clinical or regulated decisions?
- What happens if model performance shifts over time or the system gives a wrong result?
- What human review has to happen before anyone acts on the output?
Clinical AI tools need a deeper review. That means PHI handling, access controls, audit logs, retention, drift, bias, and failure modes should all be checked. Administrative tools usually need a tighter PHI-and-access review.
For example, a small FQHC might use a full clinical checklist for an AI triage platform, while using a shorter review for an AI billing assistant.
You should also reassess any AI tool when there is a meaningful change in workflow, vendor terms, model version, or data use.[3][5]
Vendor oversight for ambient scribing, triage, and other AI services
Because most community healthcare organizations get AI through vendors, this review has to live inside procurement and BAA workflows.
Ambient scribes need extra scrutiny because they may involve continuous audio capture. That makes audio retention, model training limits, and breach notification timelines the top vendor questions.[4]
A regional care network, for instance, might require contract clauses that prohibit use of visit audio for general model training, mandate U.S.-based storage, guarantee 72-hour breach notice, and provide quarterly security reports.
The table below shows the main oversight points community organizations should use when reviewing any AI vendor:
| Oversight Criterion | What to Ask or Require |
|---|---|
| PHI storage location | U.S.-only hosting confirmed in writing |
| Training on customer data | Opt-out available; no default use of patient audio or transcripts |
| Audio/data retention | Configurable retention windows with documented deletion controls |
| Subprocessors | Full list of third-party providers, locations, and vetting process |
| Validation on similar populations | Evidence of testing on comparable patient demographics (e.g., rural, Medicaid, multilingual) |
| Breach notification timeline | 48–72 hours from discovery, with defined notification method |
| Audit rights | Security reports and control evidence available on request |
| Exit and rollback options | Data export rights and ability to revert to a prior model version |
Use this table to spot vendors whose retention, training, or breach terms don't fit your risk tolerance.
Using Censinet to centralize AI risk and third-party governance
Censinet RiskOps™ gives teams one place to keep vendor questionnaires, evidence such as SOC 2 reports, risk ratings, BAAs, and internal policies. That way, reviewers can see fast what applies to each tool.
Censinet AI™ gathers and summarizes vendor responses and supporting documents, then sends key findings and remediation tasks to the right stakeholders, including members of the AI governance committee, through configurable workflows that keep risk teams in approval control.
A rural health network, for example, could register all ambient scribe and triage vendors in RiskOps, attach their assessments and BAAs, and use standardized approval flows to ensure every new AI feature is reviewed and documented without adding a full-time governance role.
These assessments should feed the privacy controls, staff training, and escalation rules that guide day-to-day AI use.
Day-to-day guardrails for privacy, patient safety, and compliance
Vendor review can stop bad-fit AI before launch. But once a tool is in use, the day-to-day guardrails do the heavy lifting. That work has to sit inside clinic operations, not live only in a policy binder.
Data-use and privacy controls for everyday AI use
Start with least-privilege access. AI tools should show PHI only to staff who need it for their job. Clinicians may need full encounter notes. Registration staff usually need demographics and scheduling fields, not the full chart. Role-based access in AI tools should match the access model already used in your EHR. A simple quarterly review can catch inactive accounts or permission mismatches before they turn into a bigger mess.
Each AI tool that touches patient data also needs a one-page data flow map. Keep it simple. It should show:
- what the tool collects, such as audio, text, or images
- where the data goes, such as a vendor cloud or an on-premise server
- how long the data is kept
- which downstream systems receive it
This can be done during vendor onboarding with a short template, so it doesn't become a side project no one finishes.
Retention rules matter too. Raw audio from ambient scribing should have a set maximum retention window, such as 7 to 30 days, with transcripts kept only as part of the legal medical record.[7][6][2] Vendors should support auto-deletion and provide deletion logs. Their contract terms should line up with those settings. The main point is simple: these controls should fit the workflows you already use for the EHR, privacy review, and onboarding.
In 13 states and the District of Columbia, all-party consent is required before recording a clinical encounter. That means affirmative consent should be captured in the EHR before ambient recording begins. If the patient says no, recording stays off.
Workflow controls, staff training, and incident escalation
Treat AI output as advice, not the final word. Clinicians should review AI-generated notes before anything enters the record. Triage flags can support judgment, but they should not trigger automatic decisions. Coding suggestions should be approved by staff before submission, without piling on a new admin process. A short AI use matrix can help here: tool, purpose, required review, and prohibited uses, all in one place.
Training should be role-based, short, and practical. People don't need a long seminar. They need to know what to do on a busy Tuesday.
- Clinicians should know they are responsible for reviewing and fixing AI output, and they should be ready to explain AI use to patients.
- Front-desk staff should know how to document opt-outs and answer patient questions.
- Revenue cycle teams should know when an AI coding suggestion looks off.
- IT staff should know how to set access controls and what to do when a tool starts acting strangely.
Short annual or semi-annual modules inside your current compliance training are enough to cover the basics. No separate AI academy required.
It also helps to name who can suspend a tool. In many clinics, that will be the medical director, privacy officer, and IT lead. Any staff member should be able to report a concern, but a named decision-maker should approve the actual suspension within a set time window. Write down the triggers. Repeated documentation errors, signs of bias, suspected data leakage, unexplained vendor changes, or patient complaints that look credible should all count.
Incident reporting should use the system you already have. Add a few AI-specific fields to the current form: tool name, date, issue description, whether an AI output was overridden, and any patient impact. Send those reports to the governance group monthly, or right away if patient safety is on the line. That makes patterns easier to spot. If a scribe keeps getting medication lists wrong, for example, that can lead to a vendor review, a policy change, or retraining. In plain terms, the loop closes back into governance instead of dying in someone's inbox.
Conclusion: Build AI governance that is realistic, defensible, and built to last
Community healthcare needs AI governance that is small, workflow-based, and firm enough to protect privacy, safety, and compliance without turning into a full-time program. That's the kind of governance small teams can keep up with.
FAQs
Where should a small clinic start with AI governance?
Small clinics don’t need a big AI program to manage risk. Start with simple controls that match your current staff and budget.
- Create an AI inventory of the tools already in use
- Assign one owner to each tool
- Rank tools by risk, and start with workflows where mistakes could cause the most harm
- Require a BAA for tools that handle Protected Health Information
- Require human review for high-risk clinical outputs
How can we review vendor AI tools without adding a new program?
Fold vendor AI reviews into the workflows you already use instead of spinning up a separate program. Keep a living AI inventory that lists each tool, its owner, and its intended use. Then assign a risk tier so you can focus the closest review on tools that touch ePHI, shape clinical decisions, or affect patient safety.
For vendor tools, put contract review first. Confirm there’s a signed BAA in place, block unauthorized data use for model training, require notice of material changes, and spell out simple stop rules plus human review requirements.
Which AI uses require mandatory human review?
Mandatory human review is a must for any AI tool where mistakes could lead to serious patient harm, legal or regulatory risk, or data privacy issues.
That applies to tools used for clinical diagnosis, triage, treatment planning, documentation, and claims processing. In plain terms, if an AI system generates notes, clinical guidance, or care recommendations, a clinician should check them before anything is finalized, signed, or used in patient care.
