AI mistakes can turn into patient harm fast. When an AI tool gives a bad answer, goes down, or quietly slips over time, care can slow, handoffs can fail, and patients can get the wrong treatment or no treatment at all.
If I had to sum up the article in plain English, it comes down to this:
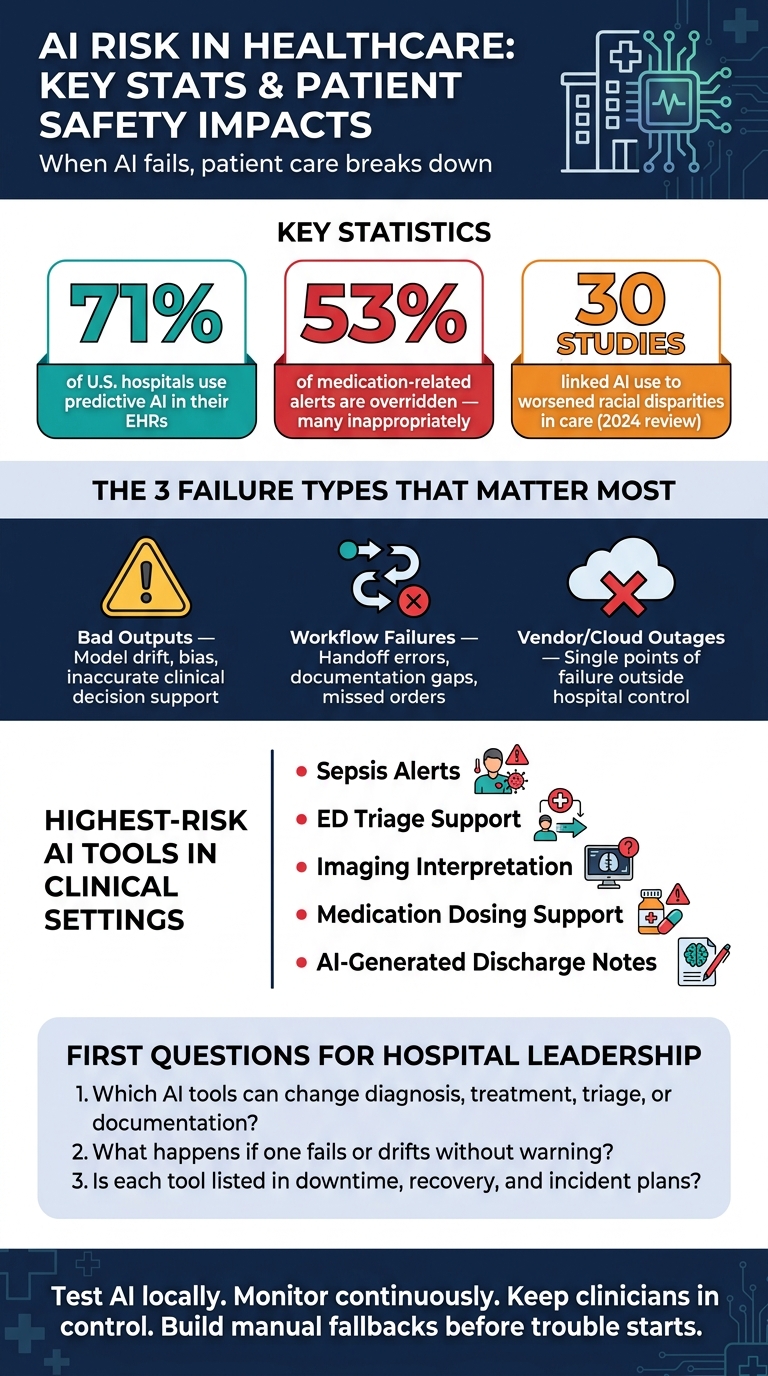
- AI risk is now a patient safety issue, not just an IT issue
- Three failure types matter most: bad outputs, workflow failures, and vendor/cloud outages
- Three parts of care get hit: care flow, information flow, and day-to-day service flow
- The highest-risk tools are the ones tied to triage, sepsis alerts, imaging, medication support, and discharge notes
- Hospitals need backup plans for when AI tools fail, not just plans for when the EHR fails
- Managing third-party AI risk remains your responsibility if it harms care
A few facts make the point clear:
- 71% of U.S. hospitals now use predictive AI in their EHRs
- A 2024 review of 30 studies linked AI use with worse racial gaps in care in some settings
- 53% of medication-related alerts are overridden, and many of those overrides are inappropriate
So, if I’m looking at this from a hospital leadership view, the first questions are simple:
- Which AI tools can change diagnosis, treatment, triage, or documentation?
- What happens if one fails or drifts without warning?
- Is each tool listed in downtime, recovery, and incident plans?
Here’s the short version of the article’s core message: test AI locally, watch it over time, keep clinicians in control, and build manual fallback steps before trouble starts.
This article then ties those risks to the parts of care that break first when AI goes wrong.
AI Risk in Healthcare: Key Stats & Patient Safety Impacts
AI failure scenarios that disrupt clinical continuity
Inaccurate outputs, model drift, and bias in clinical decision support
The continuity break here is diagnostic and treatment delay.
Clinical decision support tools can slip after deployment when data changes, workflows shift, or both. Model drift is that slow drop in accuracy over time.
Bias adds another layer of risk. A review of AI bias in medicine found that biased models can worsen disparities by steering decisions away from some patient groups, leading to delayed care and unequal treatment decisions.[3]
That’s why post-deployment checks matter so much. Health systems need ongoing validation, performance review by patient group, and outcome surveillance after rollout.[2][4][5][6]
The same problem doesn’t stop at clinician-facing advice. It also shows up when AI starts running parts of care delivery itself.
Workflow automation and documentation failures in care delivery
The continuity break here is handoff and documentation failure.
AI workflow tools used for scheduling, bed management, prior authorization, and order queues can create delays, cancel care, or send orders to the wrong place when something goes wrong. A small system error can turn into a missed procedure or a broken handoff fast.
AI note-generation tools carry a different kind of risk. They can misstate medications, leave out follow-up instructions, or produce incomplete discharge summaries that get entered into the EHR. Once that bad information is in the record, it can lead to medication discrepancies or handoff failures down the line. FDA guidance stresses ongoing validation and postmarket monitoring because many of these failures show up only after deployment.[2][5][6]
The risk climbs when these tools depend on outside vendors or cloud-based services.
Third-party AI dependencies, outages, and cyber events
The continuity break here is service interruption and outage.
A lot of healthcare AI relies on cloud-hosted models, vendor-embedded algorithms, and external APIs. That creates single points of failure outside a health system’s direct control. If a vendor service goes down, a security incident blocks access, or a model gets updated without enough notice, the clinical tools tied to it can fail without warning.
Vendor outages and cyber incidents can ripple across both clinical and operational workflows. AI-dependent services can create the same kind of fragility. That’s why third-party vendor risk management should require validation evidence, update notices, performance reporting, and bias disclosures.[2][5][6]
sbb-itb-535baee
Risk management controls that reduce patient safety and continuity risk
AI governance, validation, and continuous monitoring
These failure modes call for controls that cut both patient harm and care disruption.
A formal AI governance committee should approve, tier, and retire clinical AI tools. That group should be chartered across patient safety, quality, cybersecurity, and enterprise risk, with input from nursing, compliance, legal, IT, security, data science, and risk.
A central AI inventory - a registry of every AI or algorithmic tool in use, whether vendor-supplied or built in-house - should record the use case, data sources, deployment environment, and whether the system can directly affect diagnosis, treatment, triage, or documentation. From there, risk tiering sets the level of control. An AI sepsis predictor that triggers rapid response activation carries much more risk than a coding suggestion tool, so it should face stricter validation, continuous monitoring, and human-in-the-loop safeguards.
Local validation is the gate before go-live. Testing AI performance on your own patient population - with subgroup analysis by patient subgroup - can catch bias that top-line metrics may miss.[3][11] After deployment, teams should track override rates, alert acceptance, and error rates on recent cases, with automated alerts when metrics drift.[2][4][5][6]
Human-in-the-loop safeguards and downtime procedures
For high-impact use cases - ED triage, imaging interpretation, sepsis prediction, medication dosing, and AI-generated clinical documentation - clinicians must keep override authority. Just as important, that authority has to exist inside the workflow, not sit buried in a policy document.[3][8][9][12] Confidence indicators can help clinicians weigh recommendations instead of accepting them on autopilot. Clear escalation thresholds also matter, along with clear documentation of who needs to act.
AI-dependent workflows also need backup paths. That includes paper order sets, manual triage criteria, non-AI documentation templates, and outage alerts that reach staff fast through EHR alerts, secure messaging, and unit announcements.[7][10][1] If a tool is down or degraded, people need to know right away. Regular drills give teams a chance to practice manual workflows and spot gaps before a live outage does it for them. Post-event reviews should feed findings back into risk registers and continuity plans.
Internal downtime readiness only goes so far if third-party AI services are not held to the same safety and uptime standards.
Third-party AI oversight through contract and assessment controls
Vendor assessments for AI tools should cover a short list of core areas:
- Information security controls and HIPAA compliance
- Model validation evidence - study design, performance metrics, populations tested, and known limitations
- Bias testing results
- Change management processes for model updates
- Uptime commitments and incident notification timelines
- Audit logs for inputs, outputs, and decision paths
Contract language should make these expectations enforceable. Key clauses include uptime SLAs with remedies for prolonged outages, advance notice for major model changes, prompt incident notification duties, audit rights, and termination rights if safety or compliance standards fall short. Quarterly vendor review meetings with clinical, IT, and risk stakeholders help keep oversight active instead of turning it into a one-time procurement task.
Censinet RiskOps™ centralizes third-party AI risk assessments and maintains AI risk registers, giving teams a single source of truth that links structured assessment data to specific AI use cases and business owners - so accountability is easier to see and prioritization is easier to act on.
Connecting AI risk management to continuity planning and operations
Include AI-dependent services in business and clinical continuity plans
Once AI controls are in place, continuity planning decides what happens when those controls break down. In healthcare, that question isn't abstract. It affects whether care keeps moving or stalls out.
Most healthcare organizations already have business continuity plans. The gap is that many of those plans still haven't been updated for AI-dependent care.
Start by listing every AI-enabled workflow in the BIA. That includes ED triage, ambient documentation, imaging interpretation, prior authorization, and medication support. For each one, document:
- Maximum downtime
- Manual fallback
- Staffing impact
- Whether the workflow affects diagnosis, treatment, documentation, or patient communication
That level of detail matters. It helps teams avoid delayed diagnoses, unsafe treatment, and documentation gaps. The Joint Commission's sentinel event alert expects downtime procedures that sustain clinical continuity for up to four weeks, not just a few hours.[13][14]
Ownership also needs to be crystal clear. Assign named owners for patient impact, technical recovery, security containment, and escalation. Every AI workflow should have a business owner and a backup. When an AI tool fails, the damage shows up in the clinic, not just in the server room.
Cyber incident response playbooks should also include AI-specific actions. Spell out who declares downtime, how staff get notified, what backup process starts, and what validation must happen before the tool is cleared for clinical use again. Without that, teams can end up guessing in the middle of a live issue, and that's when mistakes pile up fast.
Use centralized visibility for AI risk, remediation, and accountability
Those playbooks are only as good as the visibility behind them. If AI risk data lives across spreadsheets, tickets, and email threads, teams lose sight of what's happening right when they need a clear picture most.
A single system of record should track AI inventory, policy status, validation findings, open remediation tasks, incident timelines, and accountable owners in one place. During an AI outage or model issue, that shared view gives clinical, technical, security, and vendor teams the same set of facts. Instead of chasing updates, they can focus on response.
Censinet RiskOps™ can fill that role as a central hub. Its AI risk dashboard pulls together current policy, assessment, and task status, while built-in routing sends findings to the right stakeholders - including AI governance committee members - for review and approval.
From Deployment to Oversight: Strengthening AI Risk Management and Patient Safety in Health Care
Conclusion: Practical priorities for protecting care delivery from AI-related harm
AI risk in healthcare isn't some far-off issue. It's already part of care delivery. Seventy-one percent of U.S. hospitals now use predictive AI in their EHRs[16]. So the job in front of health systems is pretty clear: focus first on the tools that matter most, test them on local patients and workflows, watch them over time, and keep a close eye on vendor risk.
Start with the tools that touch patients most directly and carry the most clinical weight: sepsis alerts, triage, diagnostic support, and medication safety. These are the places where mistakes can lead straight to delayed care, missed diagnoses, unsafe treatment, or documentation gaps. And the more time-sensitive the decision, the tighter the guardrails need to be. That means stronger validation, closer monitoring, and reliable fallback steps when the tool doesn't perform as expected. That's how adoption stays safe.
Every AI tool should be tested on your own patients, in your own setting, with your own workflows. Then it needs to be watched on a continuous basis for drift, subgroup bias, alert fatigue, and clinician workarounds. A model can perform well in one health system and still fall short in another. Different patient populations, different staffing patterns, different workflows - it all matters. A one-time validation check is not a safety program.
Monitoring also has to be usable in practice. If staff spot a problem, they need to be able to do something about it right away. Clinicians should stay in control, with both the authority and the training to question or override AI output, especially in diagnosis, treatment selection, and discharge planning. When 53% of medication-related alerts are overridden - and many are inappropriate[15] - that points to problems in both tool design and staff training. And when that gap grows, workflow reliability and clinician trust take the hit. This oversight also needs backup: tested downtime procedures, so if an AI tool fails, care keeps moving.
Third-party AI doesn't shift the burden away from your organization. You still own the outcome. That's why contract terms, audit rights, incident reporting rules, and clear performance expectations matter so much. Those are the tools that keep outside AI visible and under control, helping prevent outages, unsafe model changes, and clinical disruption. Expand AI use only when safety controls, monitoring, and downtime paths have already been tested and shown to work.
FAQs
How can AI errors directly harm patients?
AI mistakes can put patients at risk by weakening clinical decision-making, triage, and treatment. When data drifts, bias slips in, or system integrations fail, the result can be output that sounds confident but is simply wrong. That can lead to misdiagnoses or unsafe medication recommendations.
The danger grows when clinicians lean too heavily on those outputs. In that case, patients may face delayed care, missed conditions, or the wrong intervention at the wrong time.
There’s also a systems risk. Outages or cyber incidents can suddenly take away critical decision support in the middle of complex care, which puts extra pressure on care teams when timing matters most.
Which clinical AI tools carry the highest risk?
Clinical AI tools that directly affect patient outcomes - like triage, diagnosis, and treatment recommendations - carry the highest risk.
Triage systems sit near the top of that list. If they assign the wrong acuity level, care can be delayed. And when that happens, a patient’s condition can worsen fast, sometimes with fatal results.
Diagnostic support models bring a different kind of risk. They can miss subtle conditions that a clinician might need flagged early. Treatment recommendation engines can also cause harm, especially if they suggest unsafe dosages for underrepresented groups.
That’s why these tools need strict governance, formal validation, and continuous monitoring. In this area, there’s very little room for error.
What should hospitals do when an AI tool fails?
When an AI tool fails, hospitals need to move fast to protect patient safety.
If a tool becomes unsafe or starts to drift, the first step is simple: take it out of the workflow. That can mean suspending it, overriding it, or shutting it down until the issue is under control.
At the same time, teams should switch to tested downtime procedures so care keeps moving without disruption. Patients still need steady, safe treatment, even when the software stumbles.
Before the tool goes back into use, hospitals should investigate the root cause. What failed? Was it bad data, model drift, a system issue, or something else? You want answers before the tool touches patient care again.
And throughout all of this, human oversight matters. Clinicians should be able to override weak or unreliable recommendations at any point. When the system gets shaky, human judgment has to lead.
