If your cloud provider can read your PHI, your encryption plan has a gap. For healthcare delivery organizations, cloud key management comes down to five first steps: keep keys separate from data, use customer-managed keys for PHI, limit key access, rotate keys on a set schedule, and keep audit proof ready.
I’d sum up the article like this: encryption only works when key control stays tight. The piece ties that idea to HIPAA, NIST, HITRUST, and FIPS; shows how to set up DEKs, KEKs, root keys, HSMs, and KMS tools; compares centralized, federated, and hybrid models; and lists the top failure points, from plaintext keys in code to missed rotation and key deletion. It also points to the business risk: the average U.S. healthcare breach cost hit $7.42 million in 2025, and one OCR settlement cited $150,000 tied to static, unrotated keys.
If I were reading this for fast answers, here’s the short version:
- Use CMKs for all PHI workloads, including EHRs, backups, imaging, analytics, SaaS apps, and IoMT pipelines
- Keep a three-tier key structure: DEKs, KEKs, and root keys in a FIPS-validated HSM
- Use envelope encryption so you can rewrap DEKs without re-encrypting all data
- Prefer AES-256-GCM for data at rest and TLS 1.3 for data in transit
- Rotate KEKs at least every 90 days for high-sensitivity PHI and check logs to confirm it happened
- Enforce least-privilege IAM and MFA for anyone with key access
- Track
CreateKey,DeleteKey, and decrypt events with both alerts and monthly manual review - Keep a Key Management Policy and key inventory with owners, dates, algorithms, and review records
- Test recovery and revocation so you know what happens if a key is lost or exposed
- Use independent review so the same team does not create, approve, and audit keys
Here’s the core point in one line: the article is less about turning on encryption and more about proving who controls the keys, how they are used, and what happens when something goes wrong.
This gives you the full map before the article gets into the details.
Getting Started with Cloud KMS | Google Cloud Key Management Service Tutorial
sbb-itb-535baee
Regulatory and Framework Requirements for Cloud Key Management
Cloud key management sits under healthcare security rules. If you map each framework to one shared control set, you cut duplicate work and reduce audit gaps. In plain terms, HDOs need to map cloud key controls to clear compliance evidence, not just turn on encryption and call it done. That mapping also lowers enforcement and audit risk because it gives auditors a direct line from policy to the control that’s live in the environment.
How HIPAA, NIST, and HITRUST Apply to Key Management
The HIPAA Security Rule does not flatly require encryption, but it does require HDOs to assess it as a safeguard. The Technical Safeguards under 45 CFR Part 164.312 tie straight to key management choices:
| HIPAA Requirement | Key Management Control | What to Implement |
|---|---|---|
| Access Control & Authentication (164.312(a) + (d)) | IAM permissions and strong key access and identity controls | Restrict key access; require MFA for all key users; automate rotation on role changes |
| Audit Controls (164.312(b)) | Activity logging | Enable CloudTrail or equivalent; conduct monthly log reviews |
| Encryption at Rest & In Transit (164.312(c) + (e)) | Encryption standards and transmission security | Protect data integrity with authenticated encryption and integrity checks; encrypt PHI across all cloud data transfers |
| Contingency Planning (164.308(a)) | Key backup, escrow, and recovery procedures | Test key loss and compromise scenarios |
One clinic settlement shows what weak key control can cost: $150,000 paid to the OCR after former employees used static, unrotated encryption keys to exfiltrate patient records [2]. The takeaway is blunt: access revocation and rotation are control requirements, not optional cleanup work.
HIPAA sets the obligation. NIST shows what implementation and documentation should look like. NIST SP 800-57 covers key lifecycle management practices, including cryptographic periods, which define the approved lifetime of a key. NIST SP 800-53 SC-12 requires documentation for key generation, distribution, and protection in the System Security Plan (SSP).
Then comes validation from other frameworks. HITRUST CSF Control 09.m (Control of Keys) looks at many of the same practices, including automated rotation logs, documented destruction records, and third-party assessment reports through MyCSF [3].
FIPS Validation, Auditability, and Proof of Control
Compliance also depends on proof that the cryptographic module itself meets validated standards. FIPS 140-2 and the newer FIPS 140-3 set the security requirements for cryptographic modules. Auditors will want the NIST Cryptographic Module Validation Program (CMVP) certificate number tied to the HSM or KMS. HDOs should also verify whether software, HSM, or external key management protection is active. For PHI and other regulated workloads, HSM-backed keys are generally the right fit [3].
Proof of control comes from evidence, not statements. That usually means:
- A formal Key Management Policy (KMP) that defines generation, rotation frequency, and destruction procedures
- Immutable audit logs that show each key access event
- IAM policy exports that prove separation of duties between the KMS administrator and the database or application teams
- A cryptographic inventory listing all active keys, their algorithms, and current lifecycle status
Auditors may also run a simple but tough test: can the HDO show a key revocation test? In other words, can it revoke a key and at once make the related PHI unreadable, even to the cloud provider? For HDOs using BYOK (Bring Your Own Key) or HYOK (Hold Your Own Key), the root of trust has to stay under HDO control. That’s the line between documented key ownership and key ownership that exists only on paper.
Evidence is what turns policy into auditable control. The table below shows the evidence each framework expects:
| Framework | Control Reference | Evidence Auditors Expect |
|---|---|---|
| HIPAA | 164.312(a)(iv) | Encryption policies; configuration screenshots of PHI-containing buckets/databases showing encryption enabled |
| NIST SP 800-53 | SC-12 | System Security Plan (SSP) detailing key generation, distribution, and protection details; FIPS validation certificates |
| HITRUST CSF | 09.m (Control of Keys) | Evidence of automated rotation logs, documented key destruction records, and third-party assessment reports (MyCSF) |
| NIST SP 800-57 | Key Lifecycle Mgmt | Key Management Policy (KMP) and operational logs showing adherence to defined cryptographic periods |
| Cloud Control Matrix | EKM-01 to EKM-04 | Proof of key ownership, separation of duties, and secure key storage independent of the data storage layer |
Designing a Cloud Key Management Architecture for PHI
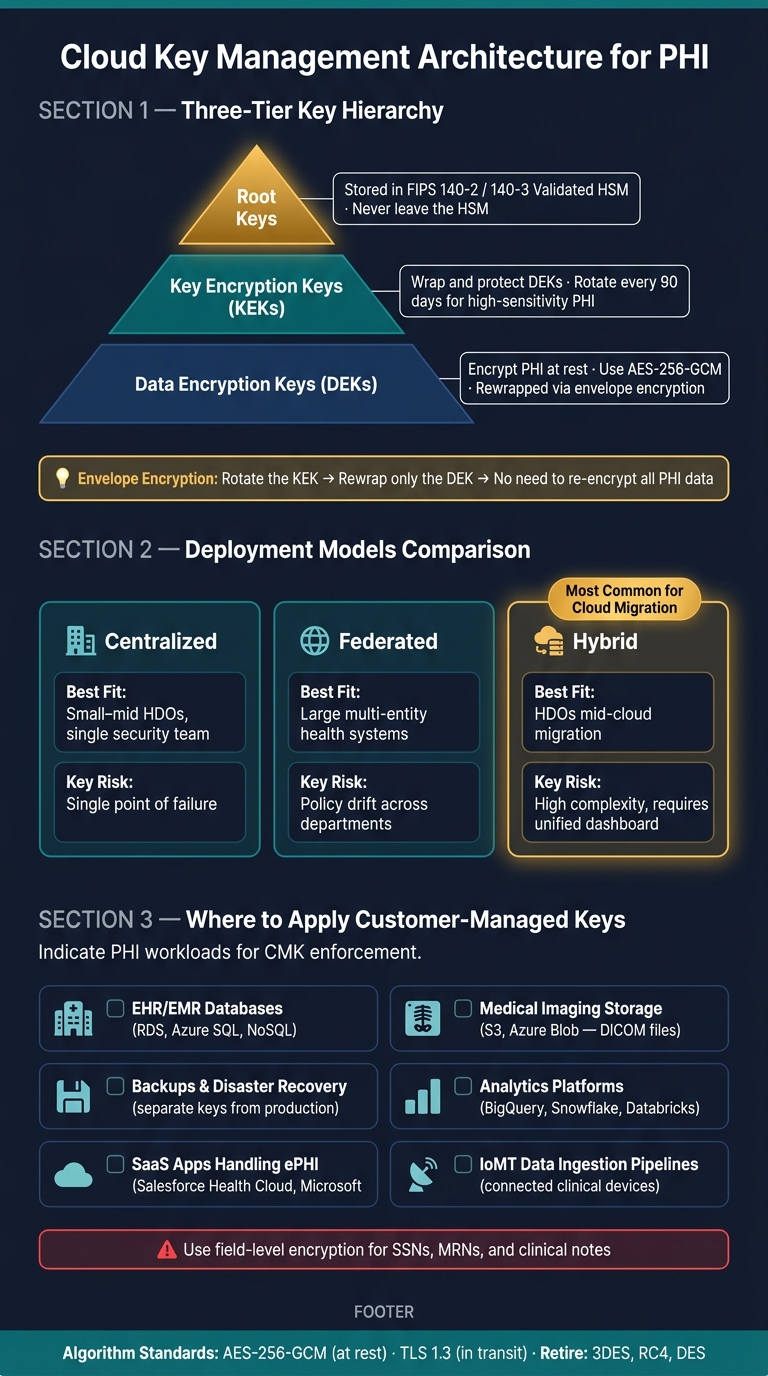
Cloud Key Management Architecture for Healthcare: 3-Tier Key Hierarchy
Once compliance requirements are set, the next step is the architecture that puts them into practice. PHI key management should enforce encryption, keep keys separate from data, and split key administration from data administration. That setup directly supports auditability, revocation, and separation of duties from the prior section.
Key Hierarchy and Lifecycle Controls
HDOs should structure encryption around three tiers: Data Encryption Keys (DEKs), Key Encryption Keys (KEKs), and root keys.
- DEKs encrypt PHI at rest.
- KEKs wrap and protect the DEKs.
- Root keys sit at the top of the hierarchy and must remain inside a FIPS 140-2 or FIPS 140-3 validated HSM.
Use envelope encryption. Store the encrypted DEK alongside the ciphertext, and when rotating the KEK, rewrap only the DEK. That keeps rotation simpler and limits exposure.
For algorithm selection, AES-256-GCM is the preferred choice for symmetric encryption of PHI at rest. For transport, TLS 1.3 is preferred, and TLS 1.2 is still acceptable. 3DES, RC4, and DES should be retired.
KEKs should rotate on a documented schedule. For high-sensitivity PHI workloads, the recommended cadence is at least every 90 days. Just as important, teams should verify completion in logs. Automation matters here because manual schedules tend to drift.
Crypto-shredding - deleting the KEK to make the data unreadable - is an effective way to make PHI permanently unreadable when a cloud service or storage layer is decommissioned.
This hierarchy shapes how easily HDOs can rotate, revoke, and recover keys without exposing PHI.
Centralized, Federated, and Hybrid Deployment Models
Architecture also depends on who controls keys across teams and environments. The right deployment model should match how the HDO governs security across sites, teams, and clouds.
| Model | Operational Benefits | Key Risks | Best Fit for HDOs | Governance Requirements |
|---|---|---|---|---|
| Centralized | Unified policy enforcement; easier auditing and compliance reporting | Single point of failure; potential latency for global clinical systems | Small to mid-sized HDOs with a single security team | Global policy defined by a central security team |
| Federated | High agility for different clinical departments or business units | Policy drift; inconsistent security posture across the organization | Large, multi-entity health systems or academic medical centers | Local oversight with central guardrails and monitoring |
| Hybrid | Maintains control of keys for highly sensitive PHI on-premises while using cloud scale | High complexity; requires robust connectivity between on-premises and cloud | HDOs in the middle of a long-term cloud migration | Unified dashboard to monitor both on-premises and cloud key usage |
For HDOs in the middle of a long-term cloud migration, a hybrid model is often the most practical fit. Legacy on-premises EHRs may stay in place while newer analytics and population health platforms move to AWS, Azure, or GCP. A hybrid architecture lets the HDO apply consistent key governance across both environments.
The next decision is where CMKs should be mandatory for PHI.
Where HDOs Should Apply Customer-Managed Keys
HDOs should apply customer-managed keys to any cloud service that stores, processes, or backs up PHI. Provider-managed keys should be reserved for non-PHI workloads.
The highest-priority workloads for CMK enforcement usually include:
- EHR/EMR databases (e.g., RDS, Azure SQL, and NoSQL environments): Core patient records need the tightest key controls.
- Medical imaging storage (e.g., S3 or Azure Blob for DICOM files): Large-volume object storage is often missed in key governance reviews.
- Backups and disaster recovery: These keys should be managed separately from production.
- Analytics platforms (e.g., BigQuery, Snowflake, or Databricks): PHI used for population health or clinical research carries the same regulatory weight as operational records.
- SaaS applications handling ePHI (e.g., Salesforce Health Cloud or Microsoft 365): BYOK is often a contract requirement for large health systems, which lets the HDO revoke access on its own.
- IoMT data ingestion pipelines: Connected clinical systems generate continuous PHI streams, so each ingestion point needs clear key governance.
Use field-level encryption for SSNs, medical record numbers (MRNs), and clinical notes.
These placement choices cut exposure, but operational drift can still create key-management risk.
Common Cloud Key Management Risks and How to Reduce Them
Once the key hierarchy is set, the biggest danger usually isn't some rare, movie-style attack. It's day-to-day mistakes.
That's where many HDOs get exposed: the space between what policy says and what teams actually do. Key management failures show up again and again in major healthcare incidents.
High-Impact Failure Scenarios in Healthcare Environments
The worst failures are usually operational, not exotic. If teams store plaintext keys in source code or environment variables, a repo or host compromise can turn into PHI exposure fast. Over-privileged KMS access creates another problem. When app service accounts or developers have broader decrypt rights than they need, one stolen credential can open far more data than intended.
Separation of duties matters here too. Key creation, approval, and review should be split up so no one person controls the full key lifecycle.
Missed rotation is also a common audit finding. Teams may say they rotate every 90 days, but the KMS record often tells a different story. Insider misuse and unauthorized key deletion are also real concerns, especially when CreateKey and DeleteKey activity isn't reviewed on a set cadence. And lost key access can be just as damaging as a breach, because it can cause permanent data loss and clinical downtime [4].
Controls That Reduce Risk Without Slowing Operations
The best controls protect PHI without getting in the way of clinical work.
- Least-privilege IAM: Apps should call KMS for decryption. They should never handle key material directly. Add MFA for any user with key management permissions.
- Automated rotation: If KMS-managed rotation runs a 90-day cycle, the human task becomes simple: do a quarterly console check and confirm the last rotated date actually changed [1].
- Anomaly detection: Automated alerts help, but they shouldn't be the whole story. Add a monthly manual review of
CreateKeyandDeleteKeyevents in CloudTrail [4]. - Log sanitization: PHI can slip into error messages and app logs when developers don't filter it out. Use build-pipeline log filters and run PII/PHI scans against log outputs on a regular basis [1].
- Dual key custodians: Assign two key custodians, one primary and one backup, so one person doesn't control the whole lifecycle [4].
Each control should have a clear owner. During an incident, vague ownership slows everything down.
Tracking Key Management Risks in Your Cyber Risk Program
Track these failures in the risk register with named owners and detection methods. The table below maps high-priority scenarios to controls, detection methods, and owners that should be formalized in your risk program.
| Risk Scenario | Impact on PHI/ePHI | Relevant Controls | Detection Method | Mitigation Owner |
|---|---|---|---|---|
| Plaintext keys in source control or env vars | Full exposure of PHI to anyone with repository or environment access | Managed KMS/HSM; secret scanning in CI/CD | GitHub Secret Scanner; static analysis (SAST) | DevSecOps |
| Over-privileged KMS access | Unauthorized decryption of PHI by internal users or compromised services | Least-privilege IAM; RBAC; MFA for KMS | CloudTrail monitoring for unusual Decrypt calls |
IAM/Security |
| Weak or manual rotation practices | Increased exposure window if a key is compromised; loss of HIPAA safe harbor | Automated KMS rotation; envelope encryption | KMS console audit; rotation logs | Key Custodian |
| Missing separation of duties | Undetected malicious key usage or unauthorized generation | Independent audits; multi-party authorization for key deletion | Monthly manual review of CreateKey/DeleteKey events |
Compliance/Internal Audit |
| Key deletion or key loss | Permanent loss of access to ePHI; clinical downtime | Key backups; multi-region replicas; deletion waiting periods; dual key custodians | CloudWatch alerts for DeleteKey events; monthly contingency testing |
Cloud Architect / Compliance |
| Plaintext PHI in error logs | PHI exposure within observability platforms | Log sanitization; field-level encryption | Log pattern matching; SIEM alerts | Application Developers |
Each row is a separate risk item that can be tracked, assigned, and reviewed on a regular cadence. Run annual tabletop exercises for key compromise and recovery.
Governance and Continuous Oversight for Cloud Key Management
After you identify risk, governance is what keeps key controls assigned, current, and ready for audit. In cloud key management, that means continuous oversight: clear ownership, current policy, and proof that reviews actually happened.
Policies, Roles, and Operating Procedures
Keep a KMP and a key inventory that lists the owner, use, algorithm, storage location, rotation date, and next review date [4]. This gives teams one place to see what exists, who owns it, and when it needs attention.
Assign a Key Management Officer (KMO) - often an ISSO or DevSecOps lead - to own lifecycle execution and maintain audit evidence [4]. Without a named owner, key management can drift fast. One team thinks another team handled rotation, review, or deletion, and suddenly no one has.
Your incident response plan should also spell out what happens if a key is compromised. That includes containment, rekeying, and re-encryption steps for affected data [4]. If those steps aren't written down ahead of time, teams are forced to improvise during a high-pressure event.
"The Key Management Plan (KMP) is a living document, and should be reviewed and updated annually, or upon any significant system or cryptographic change." - CMS Information Security and Privacy Program [4]
Use the same governance actions across the program:
| Governance Activity | Recommended Cadence | Responsible Party |
|---|---|---|
| KMP Document Review | Annually, or upon major change | KMO / ISSO |
| Key Rotation (General) | Per the KMP schedule and risk tier | DevSecOps / KMO |
| Automated Log Monitoring | Continuous | Security operations team |
| Manual Log Audit | Monthly | Designated auditor |
| Tabletop Exercises | Annually | Security / DevOps team |
Teams should continuously monitor and review CreateKey and DeleteKey events each month [4]. Those events matter because they show when keys are being added or removed - two moments that can carry a lot of risk if left unchecked.
Annual tabletop exercises must test key-compromise recovery and ISCPs [4]. This is where process meets reality. It's one thing to have a plan on paper; it's another to walk through how the team would contain damage, rotate keys, and restore normal operations.
Audits of key management processes should be handled by independent staff to preserve separation of duties [4]. That separation matters. The people doing the work shouldn't be the only ones checking whether the work was done the right way.
Using Censinet RiskOps to Assess and Monitor Key-Related Risk
That same governance needs to extend to vendors and cloud services that handle PHI. Censinet RiskOps™ helps HDOs assess key-related risk across internal systems and vendors that touch PHI.
Conclusion: Key Controls HDOs Should Prioritize First
Start with a current KMP, named ownership, least privilege, automated rotation, and independent review. Those controls turn key management from a one-time setup into something teams can run, check, and defend day after day.
FAQs
When should an HDO use BYOK or HYOK?
Choose based on your organization’s risk tolerance, technical skill, and compliance needs.
BYOK works well if you want more admin control while still using the cloud provider’s setup.
HYOK makes sense when you need the highest level of control. With HYOK, key custody stays in an external hardware security module that sits outside the cloud provider, which can help with strict compliance rules.
How do HDOs prove cloud providers cannot access PHI keys?
Healthcare delivery organizations handle this by using customer-managed keys or hybrid setups with their own hardware security modules. When they control the encryption keys, cloud providers have little to no access to the key material.
They can also show compliance with detailed, immutable audit logs for every administrative action and access request tied to those keys. Censinet RiskOps™ supports this with automated risk assessment workflows and continuous compliance monitoring.
What should happen first after a key compromise?
First, disable the affected key version and revoke all access to it right away. Then follow your incident response plan to contain the issue.
Once the immediate risk is under control, perform an emergency key rotation to restore security and help protect sensitive patient data from unauthorized access.
