If AI can survive in a small hospital, it can probably survive anywhere.
I’d sum up the article like this: healthcare AI doesn’t fail only when a model is wrong. It fails when vendors go down, data shifts, security events hit, and staff have no backup process. That risk shows up fast in community healthcare, where teams are small, budgets are tight, and downtime can hit patient care and cash flow within hours.
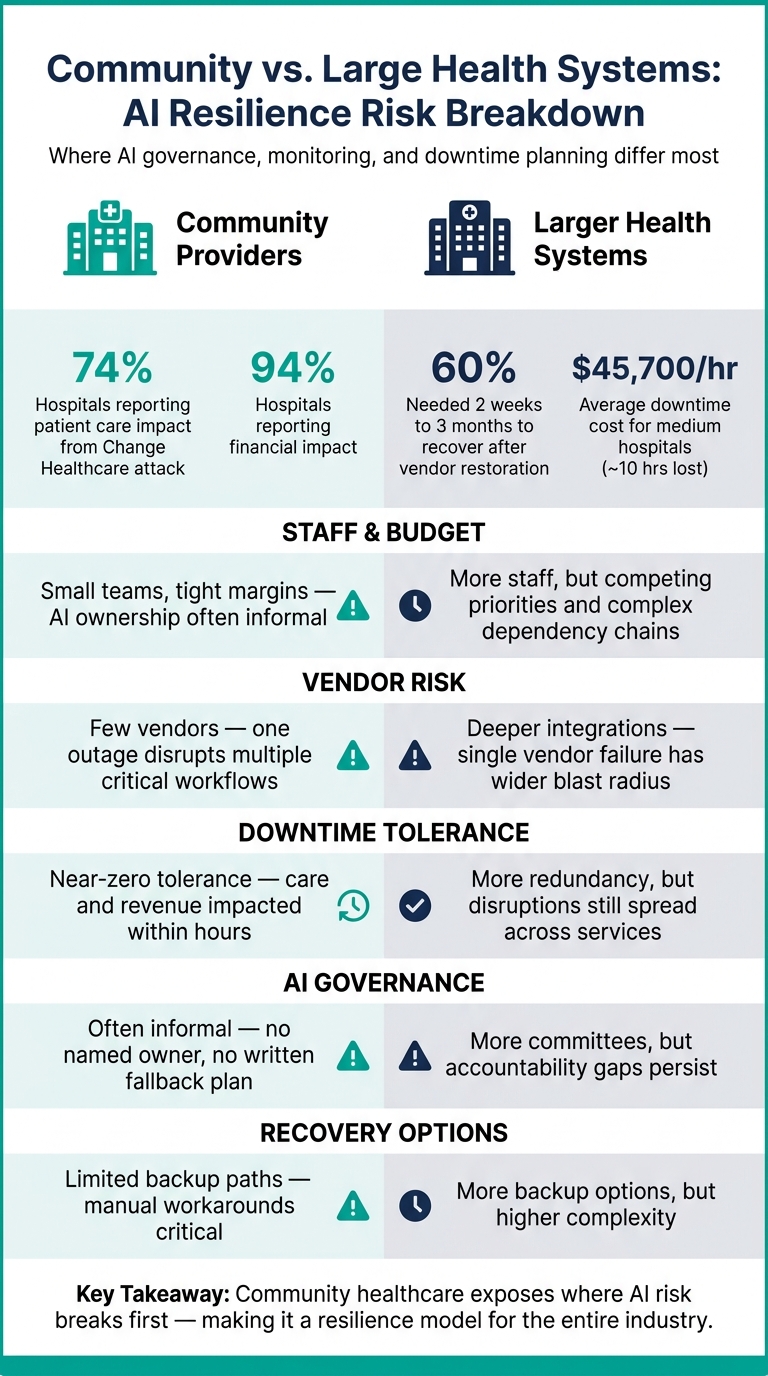
A few numbers make the point fast:
- 74% of hospitals in one survey said the Change Healthcare attack affected patient care
- 94% reported financial impact
- 60% needed two weeks to three months to get back to normal after vendor service came back
- Medium hospitals saw about 10 hours of downtime at roughly $45,700 per hour
Here’s the plain takeaway:
- AI resilience is not just model accuracy
- Vendor risk can shut down many workflows at once
- Data drift can weaken outputs little by little
- Small teams need clear owners, simple reviews, and written backup steps
- HIPAA, HITECH, and NIST already give a framework for this work
I’d also boil the article down to three actions:
- Set clear ownership for each AI tool
- Watch for drift, output changes, and security issues
- Write manual fallback plans before an outage happens
AI in Healthcare Cybersecurity: Risks, Compliance, and Practice
sbb-itb-535baee
Quick comparison
| Area | Community providers | Larger health systems |
|---|---|---|
| Staff and budget | Small teams, tight margins | More staff, but more layers and dependencies |
| Vendor risk | Few vendors, less room to switch | More integrations, larger blast radius |
| Downtime impact | Hits care and revenue fast | More redundancy, but outages can spread far |
| AI governance | Often informal | More committees, but gaps can remain |
| Recovery options | Limited backup paths | More backup options, more complexity |
My main read: community healthcare shows where AI risk breaks first. That makes it a good model for the rest of the industry. If you can set up AI governance, monitoring, and downtime plans in these settings, you have a much better shot at keeping systems safe and usable when something goes wrong.
The problem: where AI resilience breaks down in healthcare environments
Community vs. Large Health Systems: AI Resilience Risk Breakdown
AI resilience tends to fail in the places healthcare is most exposed: fragile data, vendor connections, and thin recovery capacity. So this isn't just about model accuracy. It also comes down to governance, monitoring, and what happens when the system stops working.
Cyber threats, data drift, and vendor dependency create compound failure risk
The most dangerous AI failures aren't isolated. They stack on top of each other.
A ransomware attack can hit an integration engine, cut off the data feed into an AI triage tool, and then ripple outward. Suddenly, call routing, appointment prioritization, and care escalation are all affected.
Data drift creates a different kind of risk, and it's easy to miss. If coding practices shift, patient populations change, or new devices enter a workflow, the data going into the model changes too. The model may weaken little by little, which makes the problem harder to spot. That slow decline can affect risk scoring, imaging prioritization, or utilization management before anyone realizes something is off.
Vendor dependency makes every other failure worse. If an AI vendor is compromised, outputs, integrations, and downstream workflows can all be disrupted at the same time. The ECRI Institute identified AI as the #1 health technology hazard for 2025. Bigger health systems often assume their size gives them protection. In practice, longer dependency chains and tightly connected integrations can increase the blast radius when a vendor issue hits.
Resource constraints expose gaps in monitoring, governance, and fallback planning
Many organizations still don't have a named AI owner, a change-review process, or a written fallback plan.
Governance is one of the weakest points. A lot of organizations still treat AI as an IT buying decision instead of a cross-functional risk that touches clinical leaders, compliance, cybersecurity, and operations. Without lifecycle governance, a tool may get reviewed once during purchase and then keep running without close oversight through model updates, workflow changes, and vendor incidents. Any one of those can quietly weaken reliability or create new compliance exposure.
Comparison table: community healthcare pressures vs. larger-system exposure
| Pressure point | Community healthcare reality | Larger-system exposure |
|---|---|---|
| Budget | Tight margins; limited IT and security headcount | Larger budgets, but competing priorities and more complex dependency chains |
| Staffing | Small teams wear multiple hats; AI ownership is often informal | Dedicated teams exist, but accountability gaps persist across departments |
| Vendor concentration | Few vendors; one outage affects multiple critical workflows | Deeper dependency chains; a single vendor failure carries a wider blast radius |
| Downtime tolerance | Near-zero; disruption quickly affects patient care and operations | More redundancy, but disruptions still spread across connected services |
| Change-control speed | Simpler structure, but fewer formal controls and review cycles | More committees, but reassessment lags after model updates or vendor changes |
Those gaps are only manageable when AI risk is treated as an ongoing operational control, not a one-time purchase review. The next step is building governance, monitoring, and downtime procedures that can hold up under pressure.
Solution 1: practical governance and third-party AI controls that hold up under pressure
Build small, accountable AI governance structures tied to existing committees
Start with a small AI governance group inside committees you already have. That usually means:
- a clinical champion focused on workflow fit and patient safety
- a security/IT lead focused on integrations and logging
- a compliance leader focused on HIPAA, HITECH, and BAAs
- an operations owner focused on reporting and downtime procedures
This doesn't need to turn into a big new layer of process. An IT governance committee can add an AI review segment and use a standard intake form. A patient safety or quality committee can track post-implementation metrics, incident reports, and near-misses. That same process can also be used to retire tools that drift or fall short after a vendor incident.
The payoff is simple: a clear decision log without a lot of overhead.
When no one owns the tool, no one catches the problems.
Once ownership is clear, the next move is steady monitoring and a fallback plan that has actually been tested.
Apply lifecycle-based risk reviews before adoption, during use, and at change events
Governance can't stop at go-live. Purchase review alone is not governance. Teams that hold up under pressure treat AI oversight as a continuous process with three stages.
Before adoption, review workflow fit, data quality and sources, how PHI is handled, access controls, and one direct question: "What happens if this service is unavailable for 24–72 hours?" For clinical tools, that downtime question helps define whether a fallback plan needs to be in place before go-live.
During use, track performance, complaints, error rates, and misuse. Drift tends to show up in documentation accuracy, error rates, throughput changes, and other signs that the tool is no longer doing the job you expected.
At change events, reassessment is not optional. Review again after model updates, new integrations, vendor incidents, or workflow redesigns. Community teams with small staffs can tier these reviews, with lighter checks for low-impact tools and deeper reassessments for tools that touch clinical decisions or revenue-critical workflows.
For lean teams, the goal is to make those reviews repeatable instead of starting from scratch each time.
Put governance into practice with Censinet RiskOps, Censinet AI, and Censinet AITM
Lean teams need traceable governance, not spreadsheets and scattered notes.
Censinet RiskOps keeps policies, assessments, owners, and remediation status in one system of record. That traceability helps during audits and when showing alignment with HIPAA and NIST AI RMF expectations.
Censinet AI routes intake, assigns review tasks, and requires human sign-off before implementation. That setup helps stop uncontrolled rollouts pushed by individual departments or vendor pressure.
Censinet AITM automates third-party AI assessments, ingests vendor evidence, and flags gaps. It uses prebuilt assessment templates tailored to AI use cases, covering model governance, data handling, security controls, and regulatory considerations. It also generates risk ratings, which helps teams keep assessments moving without losing discipline.
Solution 2: monitor AI continuously and design clear fallback workflows
Track model performance, drift, and bias as risk signals
Once governance is in place, resilience comes down to two things: steady monitoring and tested fallback workflows. In community settings, where teams are often stretched thin, slow detection and last-minute recovery can get expensive fast.
AI monitoring should be treated as both an operations control and a security control, not just a model-quality check. Data drift, spikes in alert volume, and output changes that no one can explain are all warning signs. You need to watch both inputs and outputs.
On the input side, that means looking at data drift, coding shifts, and workflow changes. On the output side, it means tracking accuracy, calibration, alert volume, and override rates. Accuracy by itself doesn't tell the whole story. Research on medical imaging AI shows that overall accuracy scores often miss data drift, and detection depends a lot on dataset size and which features are changing.[2]
Bias needs its own monitoring lane. A model that looked fair at launch can drift over time as patient populations change or maintenance work adds skew. One sepsis model was temporarily disabled after drift in patient characteristics led to a 43% increase in alerts, a sharp sign that drift can chip away at both reliability and equity.[9] That kind of signal should trigger a review, not just sit in a log.
For lean teams, threshold-based reviews and clinician feedback can go a long way. If a physician starts overriding AI recommendations more often, that's not noise. It's data, and it should be captured.
Prepare downtime procedures for AI-enabled clinical and administrative workflows
Plan for AI tools to fail. Then write down what happens next before that day comes.
U.S. healthcare organizations lost an estimated $21.9 billion in downtime from ransomware attacks between 2018 and 2023.[10] And because AI now touches both clinical and administrative work, each workflow needs its own fallback plan.
That plan should spell out pause criteria, manual workarounds, escalation paths, communication steps, and who owns restoration. NIST AI RMF-related guidance notes that fallback may mean manual processing, not just automated recovery.[1]
For clinical workflows, an AI-assisted triage pause means going back to nurse or physician review with rule-based protocols. Documentation shifts to manual templates or dictation. Order support returns to standard clinical decision support or direct guideline review. Imaging review moves back to conventional worklists instead of AI-ranked queues.[1][3][5]
Administrative teams need their own backup path too. Scheduling and revenue cycle staff may need to switch to manual queue management, spreadsheet reconciliation, and direct patient outreach. Standardized downtime forms, department-level go-bags with paper workflows, and named downtime teams fit naturally into AI fallback planning.[6][7][8]
Risk-impact table: failure modes, monitoring signals, and fallback actions
| Failure mode | Community healthcare safeguards | Monitoring signals | Fallback actions |
|---|---|---|---|
| Cyber compromise | Integrate AI monitoring with security event detection and incident response playbooks | Unusual output patterns, access anomalies, security alerts | Disable the tool; activate downtime procedures; notify staff; hold restoration until security review is complete[7][8] |
| Data drift | Scheduled threshold-based reviews, clinician feedback loops, input distribution tracking | Alert volume changes, rising override rates, subgroup performance shifts | Escalate through governance; run targeted validation; suspend if cause is unclear; revert to manual workflow |
| Vendor outage | Clearly defined pause criteria and workflow-specific fallback plans | Outage beyond 4 hours, failed integrations | Activate manual workarounds; communicate to affected staff; track duration; follow named restoration owner[1][2][3][4] |
| Model misconfiguration | Pre-go-live validation and reassessment after model updates or new integrations | Inconsistent outputs, calibration errors, spike in clinician complaints | Pause the tool; conduct targeted reassessment; return to service only after review and restoration approval |
These controls matter only if they line up with HIPAA, HITECH, and NIST risk expectations.
Solution 3: align AI resilience with HIPAA, NIST, and ongoing risk assessment
Map AI safeguards to HIPAA, HITECH, and NIST control expectations

Compliance and resilience are the same job with different paperwork. If an AI system touches PHI, the safeguards that keep it safe should line up with HIPAA, HITECH, and NIST.
NIST SP 800-66 Rev. 2 links HIPAA security requirements to NIST CSF and SP 800-53 controls. That gives teams a ready-to-use crosswalk, including a machine-readable version in the NIST Cybersecurity and Privacy Reference Tool. For most healthcare AI use cases, the focus comes back to three basics: confidentiality, integrity, and availability. In plain terms, that means controlling who can access model outputs and the PHI that feeds them, making training data and model settings tamper-evident and change-controlled, and making sure key workflows can keep moving if AI tools fail. Those safeguards map directly to HIPAA Security Rule requirements under 45 CFR 164.308 and 164.312.[11]
After that mapping is in place, teams should rank AI systems by patient harm, workflow criticality, and downtime cost. That helps separate a low-stakes internal tool from one that could affect care delivery. It also makes sense to track state AI rules alongside HIPAA and NIST, especially where documentation and human review come into play.[13][14][15]
Prioritize risk assessments around patient safety, critical workflows, and financial exposure
Control mapping is the start, not the finish. Lean teams still need to decide where to spend limited time and review effort.
AI systems that directly shape clinical decisions, such as diagnostic support, sepsis prediction, or triage recommendations, belong in the highest-risk tier. They need deeper and more frequent assessments. By contrast, tools used for de-identified back-office analytics can usually be reviewed on a lighter cycle. A practical way to sort this out is to classify AI assets by:
- workflow criticality
- data sensitivity
- patient harm potential
- downtime cost
That kind of triage helps resource-constrained teams focus on the tools that could do the most damage if something goes wrong.[11][12]
Financial modeling should come from internal data, not generic industry benchmarks. Say a hospital depends on an AI-powered scheduling and capacity-management tool. To estimate outage exposure, the team can add up lost or delayed appointments, overtime labor tied to manual recovery, and downstream penalties or contract effects. For example, 80 canceled visits at $1,500 each equals $120,000 before recovery costs and follow-on disruption are even counted. The point is simple: use internal assumptions and actual operating data, not rough outside averages.[12]
Conclusion: what the industry should take from community healthcare now
These controls only count if they are documented, tested, and repeatable. Community healthcare doesn't win through size. It wins through discipline.
Keep AI governance small and accountable. Treat AI vendors like core resilience dependencies. Monitor for drift and security anomalies on a steady basis. And write manual fallback procedures before anyone needs them, with documentation that maps cleanly to HIPAA and NIST expectations. Censinet RiskOps, Censinet AI, and Censinet AITM can help teams scale this work across complex healthcare settings, giving boards and risk teams a consistent, auditable view of AI risk posture over time.
FAQs
Why is community healthcare a good test case for AI resilience?
Community healthcare organizations run into the same AI risks as big health systems: bias, model drift, data exposure, and vendor dependence. The difference is simple. They usually have fewer resources, tighter budgets, and smaller teams that often don't include AI specialists.
That said, their day-to-day experience makes one thing clear: AI resilience doesn't depend on huge programs or big spending. Lean teams can handle AI risk with practical, step-by-step governance. That can mean keeping an AI inventory, sorting tools by risk level, and putting human review in place where it matters most.
What should an AI downtime plan include?
An effective AI downtime plan should protect patient safety and keep day-to-day work moving when automated systems fail. It needs to spell out who can pause, override, or shut down a tool during an incident.
It should also lay out manual backup steps for AI-dependent clinical and administrative workflows, assign response roles, and document escalation paths in your systemic risk map so teams can find them before an emergency hits.
How often should healthcare teams review AI tools for drift or risk?
Healthcare teams shouldn’t rely on one-time assessments. Drift can happen quietly, little by little, so continuous monitoring needs to be part of a lifecycle-based approach to AI governance.
Review timing should match the tool’s risk tier. Teams should also run checks when major changes happen, such as model updates, data pipeline changes, or shifts in clinical guidelines. On top of that, formal periodic revalidation - often once a year - helps confirm that the tool still fits local practice and the patient population it serves.
