AI oversight is now a board job. If AI touches patient care, billing, scheduling, records, or PHI, I need directors to treat it like a risk issue tied to quality, compliance, and security - not just an IT purchase.
Here’s the short version:
- AI use is already broad in healthcare. The article points to 71% of acute care hospitals using predictive AI by 2024, with heavy use in imaging, documentation, billing, and scheduling.
- Boards need clear ownership. I’d expect a named executive, a board committee, and a written charter with approval rules, shutdown authority, and escalation steps.
- Every AI tool needs to be listed and tiered by risk. That includes EHR tools, vendor tools, and shadow AI used by departments.
- Higher-risk AI needs tighter human review. If a tool affects diagnosis, triage, medication, or other care decisions, people must be able to review, override, and stop it.
- HIPAA, PHI, and vendor controls matter. Directors should check BAAs, data-use limits, subcontractor access, logging, encryption, and model training terms.
- Approval should be evidence-based. I’d want proof of validation on the organization’s own patients, bias checks, drift monitoring, security testing, and failure planning.
- Board reporting should not stop after launch. Directors should get regular updates on incidents, near misses, drift, override rates, vendor status, and accepted residual risk.
In plain terms, the article says a healthcare board should be able to answer five questions at any time: What AI is in use? Who owns it? What risk does it carry? How is it being watched? What has gone wrong so far?
That is the core message of the piece.
From Deployment to Oversight: Strengthening AI Risk Management and Patient Safety in Health Care
sbb-itb-535baee
Core AI Oversight Responsibilities Healthcare Directors Must Take On
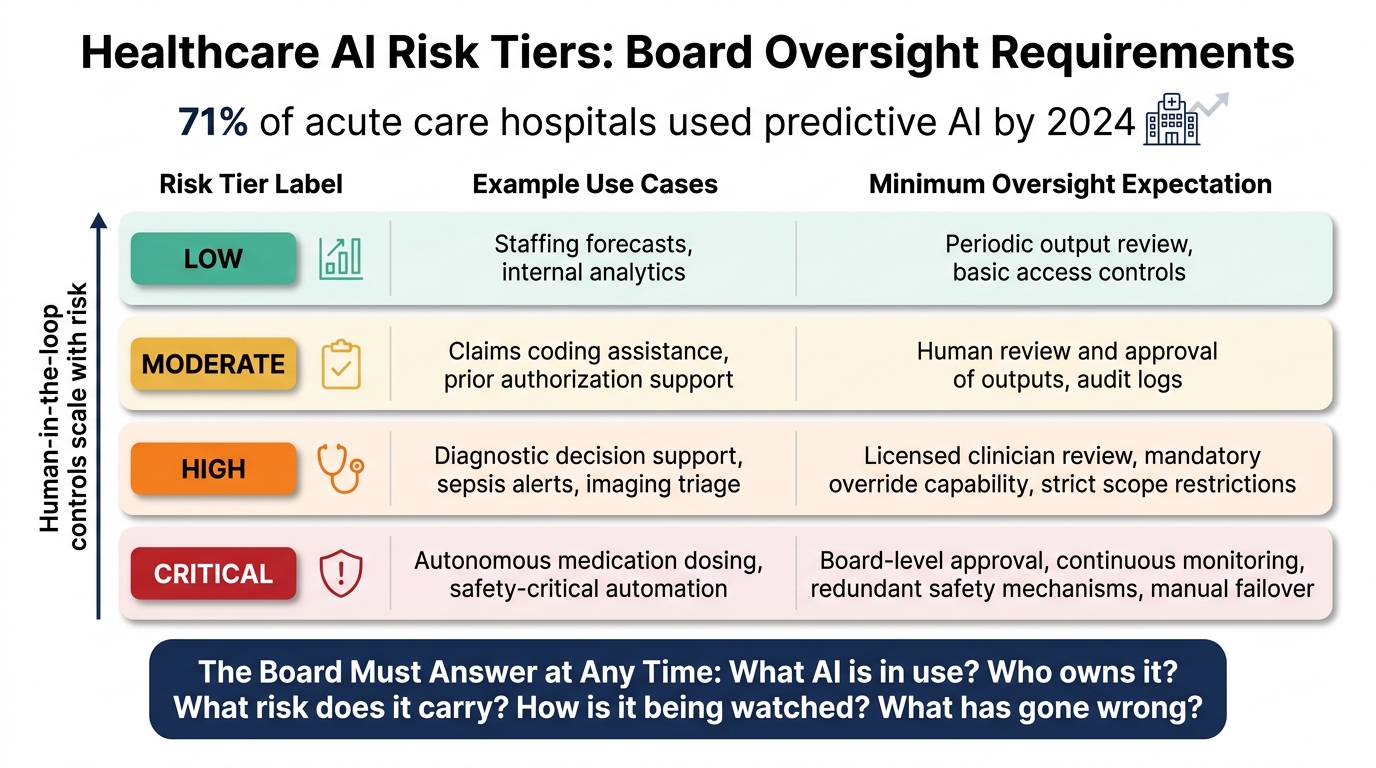
AI Risk Tiers in Healthcare: Oversight Requirements by Risk Level
Directors need to own three basics: governance, inventory, and escalation. The job is to move past broad concern and get to named oversight, a clear inventory, and controls people can actually enforce.
Require a Formal AI Governance Structure, Charter, and Named Accountability
Start with structure. Someone needs to own AI oversight, and the path for decisions needs to be plain.
Any healthcare organization using AI should have a governance charter that spells out approval rules and shutdown authority for any system that creates material safety or compliance risk. That authority should sit with a named executive, such as the CDO, CISO, or CMO, with direct responsibility for AI risk across quality, compliance, cybersecurity, and privacy.
Board oversight matters too. Assign AI oversight to a standing board committee. The charter should set acceptable risk levels, tier-based approval thresholds, escalation triggers, and clear links to HIPAA, cybersecurity, and patient-safety policies. It should also require an annual review and tabletop exercises built around actual AI incident scenarios.
Require an AI Inventory, Risk Tiering, and Human Oversight Controls
Once ownership is set, directors need a full picture of every AI tool in use.
That means requiring a centralized AI inventory that covers EHR-embedded tools, third-party vendor tools, and shadow AI picked up by departments. Without that list, directors can't tier risk or set the right monitoring rules.
Each inventory entry should record the use case, what data the tool touches, whether PHI is involved, and how the AI shapes decisions. Then tier each tool by risk.
| Risk Tier | Example Use Cases | Minimum Oversight Expectation |
|---|---|---|
| Low | Staffing forecasts, internal analytics | Periodic output review, basic access controls |
| Moderate | Claims coding assistance, prior authorization support | Human review and approval of outputs, audit logs |
| High | Diagnostic decision support, sepsis alerts, imaging triage | Licensed clinician review, mandatory override capability, strict scope restrictions |
| Critical | Autonomous medication dosing, safety-critical automation | Board-level approval, continuous monitoring, redundant safety mechanisms, manual failover |
Human-in-the-loop controls should scale with risk. For high-risk systems, directors should require an easy clinician override and EHR logging that shows whether recommendations were accepted, modified, or rejected[3][4].
Align AI Use with HIPAA, Cybersecurity, and Patient-Safety Requirements
An inventory by itself won't do the job. Directors also need compliance and security controls tied to each tool's PHI exposure.
Any AI system that handles PHI must fall under HIPAA rules. Directors should require executed Business Associate Agreements that directly address AI-specific data use, including limits on model training and secondary commercial use. Access controls, encryption, and audit logging are required[1][2].
Directors should also make sure AI is part of cybersecurity risk assessments. That includes AI-specific threats such as prompt injection, data poisoning, model drift, model extraction, and sensitive data leakage caused by misconfigured integrations or overly detailed outputs[2][3][7][8]. A cyber failure in AI can turn into a clinical failure fast. Directors should ask for proof that management has mapped these threats and tested the controls.
Oversight Questions Directors Should Ask Before Approving AI
Once governance and inventory are in place, directors need a short set of approval questions that force management to show proof, not just give broad assurances. Put simply, if an AI tool is going to affect care, patients, or payment decisions, the board should expect evidence before it signs off.
Questions on AI Inventory, Clinical Impact, and Failure Modes
Start with the basics: which AI tools are already in production, which are still in pilot, and which affect clinical, patient, or payer decisions? That review should cover internal tools, vendor products, embedded AI inside current software, and any shadow AI picked up outside formal governance.
Then get clear on purpose and limits. Ask what the tool is meant to do, and just as important, what it is not meant to do. Ask what happens if the model misses a condition, overcalls a finding, or performs differently across patient groups. If management can't clearly name failure modes, the tool should not be approved. Directors should also confirm that AI-related adverse events and near misses go to clinical leadership for review.
After scope is clear, the next step is simple: does the model actually work for your patients?
Questions on Validation, Monitoring, and Bias Controls
Ask whether the AI was validated on the organization's patient population, not only on the vendor's test set. A model can look accurate in testing and still fall apart at the bedside if the patient mix differs from the vendor's test cohort.
Monitoring matters just as much as initial testing. Ask whether monitoring is continuous or one-time. Ask what thresholds trigger a review if performance drops, how drift is detected, and who gets alerted when model behavior changes. On bias, ask which subgroups were part of testing, whether any performance gaps showed up, and whether bias monitoring continues after deployment.
If the tool is vendor-managed, board review also needs to cover contract terms and escalation rights.
Questions on Vendors, PHI Handling, and Escalation Paths
Confirm that a BAA is in place and that the contract spells out data use, including whether the vendor can train on organizational data. Ask for independent security assessments, not only vendor self-attestation. And ask about downstream subcontractor access. Do the same data-use restrictions apply to subcontractors too?
This is bigger than paperwork. Directors are deciding who has the authority to stop risk, not just who wrote the vendor controls into a contract. Ask who owns the escalation path from operational teams to clinical leadership, compliance, cybersecurity, and the board when a serious AI issue occurs. Require tabletop exercises that test escalation, not just a policy sitting on a shelf. Ask who is accountable for keeping the tool running - or suspending it - if it fails tomorrow.
| Risk Domain | Key Director Questions | Committee Ownership |
|---|---|---|
| Inventory & Clinical Impact | Which tools are in production or pilot? Which influence clinical, patient, or payer decisions? | Quality / Patient Safety |
| Failure Modes | What are the known failure modes? How are AI-related adverse events escalated? | Quality / Patient Safety |
| Validation | Was the tool validated on our patient population? Is monitoring continuous? What triggers a review? | Audit / Risk / Compliance |
| Bias | Which subgroups were tested? Were gaps found? Is bias monitored post-deployment? | Audit / Risk / Compliance |
| Vendor / PHI | Is the BAA AI-specific? Does it prohibit vendor training on our data? What is the downstream subcontractor access? | Cybersecurity / Privacy |
| Escalation | Who decides to suspend the tool? Has escalation been tested in a tabletop exercise? | Cybersecurity / Privacy |
How Directors Can Put AI Risk Assessment and Vendor Oversight Into Practice
Directors need more than answers to oversight questions. They need a repeatable AI risk review that leads to documented approvals. The next move is a standard review process that turns those questions into decisions the board can track.
Set Minimum AI Risk Assessment Criteria for Internal and Vendor Tools
Use the NIST AI RMF as the board’s review structure: GOVERN, MAP, MEASURE, MANAGE. For every intake, require documentation on ownership, intended use, patient impact, validation, monitoring, and decommissioning triggers. [5][9][11]
The same baseline should apply to internal tools and vendor tools.
| Assessment Area | Internal AI Tools | Third-Party Vendor AI |
|---|---|---|
| Intended use & risk tier | Documented design assumptions, training data scope, deployment context | Formal indications for use, FDA status, stated limitations from vendor labeling |
| PHI handling | Data lineage, source systems, preprocessing pipelines, internal data-use approvals | Disclosure of PHI use for training, data residency, encryption standards, customer data segregation |
| Access control & logging | Role-based access, MFA, integration with internal IAM, audit logs for inputs/outputs | SSO/SAML support, granular authorization, exportable audit logs to customer SIEM |
| Validation evidence | Internal validation on a local patient cohort, simulation or pilot data | Peer-reviewed or field performance summaries, performance by subgroup |
| Adversarial & bias testing | Internal robustness testing, bias review across protected classes | Vendor-supplied bias testing results, mitigation steps for identified disparities |
| Contingency plan | Rollback procedures, manual fallback workflows, root-cause analysis responsibilities | Uptime and support SLAs, vendor incident notification timelines, cooperation obligations |
| Residual risk documentation | Signed acceptance by the CMO, CISO, Compliance Officer, and business owner | Residual risk statement in the board packet, conditions on approval documented in committee minutes |
A diagnostic vendor review shows what this looks like at the board level.
A Diagnostic Vendor Review as a Board-Level Example
For a diagnostic AI review, require six artifacts: regulatory status, validation evidence, workflow map, human override points, third-party security review, and residual risk documentation. [10]
- Regulatory status: Confirm clearance status, intended use, and labeling. Flag any off-label use for clinical governance review.
- Validation evidence: Require performance metrics - sensitivity, specificity, AUC, and calibration - broken down by age, sex, and race, not aggregate numbers alone.
- Workflow map: Show where the AI output appears in the clinical workflow and who acts on it, including how conflicting results between the AI and a clinician are resolved.
- Human override points: Document every point where a clinician can override the AI, and flag any scenario where the system acts autonomously.
- Third-party security review: Require an independent assessment covering encryption, access controls, penetration testing, and breach notification timelines.
- Residual risk documentation: Before approval, a written residual risk statement must name known limitations, link each to a mitigation measure, assign a risk level, and carry signatures from the CMO, CISO, and Compliance Officer. That document belongs in the board or committee minutes, along with any conditions placed on the approval.
Think of these six items as the board’s case file. If one is missing, the review is incomplete. That’s how directors avoid vague sign-off and get a clear record of what was reviewed, what was accepted, and what still needs a guardrail.
Those artifacts should live in one system of record for board reporting and audit readiness.
Centralize Workflows and Evidence with Censinet RiskOps and Censinet AI
Route AI risk assessments through Censinet RiskOps™ as the system of record for questionnaires, routing, evidence, and approvals. Use Censinet AI™ to draft summaries and board materials, with every output reviewed by a named human approver before it reaches the board. [10]
Building Continuous AI Oversight Into Board Reporting and Governance
AI oversight can't be a one-time approval. Once a tool goes live, performance can drift, data can change, and vendor behavior can shift.
That means oversight needs to be continuous, documented, and built into the governance work the board already does.
Add Regular AI Reporting to Quality, Audit, Risk, and Cyber Reviews
AI reporting should be a standing board agenda item. The Joint Commission calls for regular board updates on AI use, outcomes, and adverse events, folded into current compliance, risk, and patient-safety structures.[12][13]
Put simply, approval is the start. Ongoing committee reporting is what turns that approval into control.
| Committee | Core AI Metrics | Cadence | Decision Rights |
|---|---|---|---|
| Quality & Patient Safety | AI-related adverse events, near misses, clinical performance drift, clinician override rates | Quarterly | Approve changes to clinical AI deployment |
| Audit & Compliance | Inventory completeness, PHI-handling controls, HIPAA alignment, open remediation items | Quarterly | Require corrective action plans, flag regulatory exposure |
| Enterprise Risk | Risk register updates, residual risk decisions, vendor reassessment status, escalation threshold breaches | Quarterly | Accept residual risk, require mitigation plans |
| Cybersecurity / Technology | PHI incidents, AI-related security events, uptime impact, vendor security reassessment results | Monthly and ad hoc for material incidents | Approve technical control changes, escalate breaches |
Each cycle, those committee updates should roll up into one board summary. That gives directors one clear view instead of bits and pieces spread across meetings.
Document Residual Risk Decisions and Update Policies as Standards Change
Reporting has to lead somewhere. If monitoring shows a shift in performance or risk, the board needs a clear, written path for re-review, escalation, and policy updates.
Every accepted residual risk should have a written record and a trigger for re-review. Record the risk, likelihood, impact, mitigation, acceptance rationale, escalation threshold, and approver names and dates.[6][14][15]
That kind of record matters when someone asks hard questions later. It helps make board risk decisions defensible to OCR, to the FDA for regulated devices, and to internal or external review. It also keeps accountability clear across clinical and operational teams.
Review charters and policies every year and after major changes in NIST, FDA, OCR, or Joint Commission guidance.[6][5][16] Assign a standards owner in compliance, the Chief AI/Data Officer, or a designated committee to alert the board when guidance changes.
Key Takeaways for Directors Preparing Now
Directors don't need to wait for a new rule or a patient-safety event to put real AI oversight in place. The most important steps right now are pretty straightforward:
- Treat AI as a board-level risk and name accountable executives. Add AI to the enterprise risk register and to each relevant committee charter. Spell out how named executives - such as the CMIO, CIO, CISO, CCO, or Chief AI/Data Officer - report to the board.
- Maintain a complete, risk-tiered AI inventory. Every tool, whether built inside the organization or supplied by a vendor, should have a named owner, a documented use case, PHI use, and a validation status.
- Use standing committee reporting and re-review triggers. Track clinical performance, bias, PHI incidents, and vendor status on a set cadence, and require written re-review when escalation thresholds are crossed.
- Centralize approvals, monitoring evidence, and vendor records. Route assessments, approvals, and board materials through one system of record so oversight can be audited across the full AI lifecycle.
A board should be able to answer, at any time, what AI systems are in use, who owns them, what risks have been accepted, what monitoring is active, and what incidents have occurred. That's what actual AI governance looks like.
FAQs
How should boards prioritize AI risks?
Boards should start by setting clear ownership. Each AI system needs an executive owner with the power to approve it, watch its performance, and pause or retire it if safety issues show up.
From there, management should sort AI tools into risk tiers based on clinical impact, data sensitivity, and how deeply they’re woven into daily workflows. That way, higher-risk clinical tools get more testing and review from people across different teams.
AI governance isn’t a one-and-done checklist. It needs regular oversight as systems change, data shifts, and new risks come into view.
Who should own AI oversight internally?
AI oversight works best with two layers of accountability.
The board carries final responsibility. At the same time, a named senior executive who reports to the CEO should handle day-to-day authority. That person should have the power to approve, monitor, pause, or retire AI systems when needed.
Execution should be backed by a multidisciplinary governance committee. In plain terms, this is the group that helps turn policy into action. Roles should be clear across clinical leadership, IT and informatics, security and privacy, legal and compliance, procurement, and operations.
What evidence should directors require before approval?
Before approving an AI tool, directors should ask for a documented evidence package - not just a sales pitch from the vendor. That package should show how the tool performs on the organization’s own patient population and inside its actual workflows.
Include:
- clinical safety, workflow fit, and demographic bias testing
- model documentation, failure modes, and FDA status or exemption
- monitoring, drift, incident response, and rollback plans
- a BAA, HIPAA compliance evidence, and named business, clinical, security, and privacy owners
