If your hospital can’t tie a device flaw to a device, a patient setting, and a response owner fast, reporting breaks down.
I’d sum this article up like this: HDO IoT vulnerability reporting needs five things working together - asset inventory, standard intake, clinical context, stakeholder communication, and incident response linkage. That matters more now because healthcare IoT spans medical devices, building systems, and other connected equipment, while rules from the FDA, HIPAA, CIRCIA, and NIST add filing and documentation pressure.
A few points stand out right away:
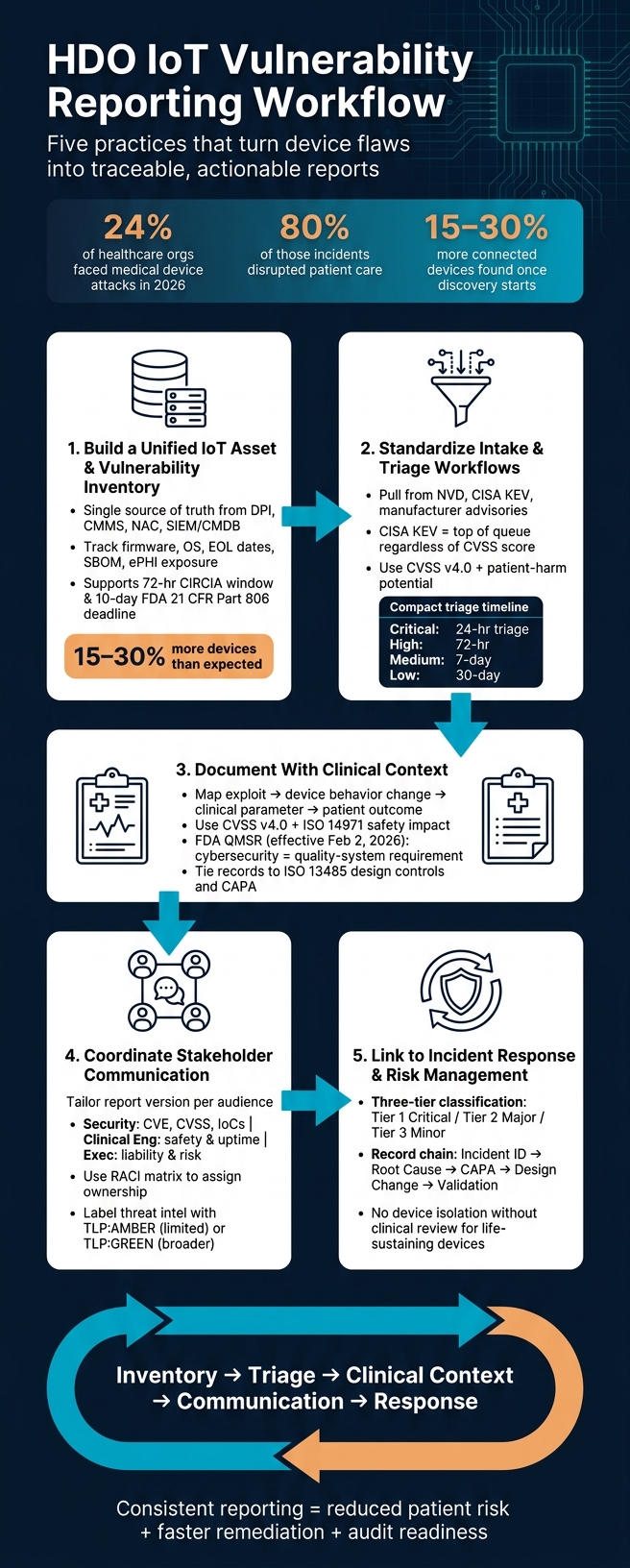
- 24% of healthcare organizations faced attacks aimed at medical devices in 2026
- 80% of those incidents disrupted patient care
- Many hospitals find 15–30% more connected devices than expected once discovery starts
- Reporting has to track both security risk and patient safety risk
- Time windows like 72 hours for CIRCIA-related incident reporting can be hard to meet without clean records
If I were reducing the piece to its core message, it would be this:
- Keep one current device and vulnerability inventory
- Use the same intake and triage steps every time
- Write reports in plain language that connect the flaw to patient impact
- Send the right version of the report to the right team
- Tie each report to containment, remediation, CAPA, and audit records
This article is less about finding flaws and more about making sure each flaw turns into a usable, traceable report that supports care, compliance, and follow-up.
HDO IoT Vulnerability Reporting Workflow: 5-Step Process
Navigating the Complexity of IoT Device Vulnerability: The Future State of Medical Device Security
sbb-itb-535baee
What Every HDO IoT Vulnerability Report Should Include
Once a vulnerability is found, each report needs to record the same core details.
A vulnerability report only helps if it includes the right information from the start. If key fields are missing, teams waste time figuring out which device is affected, what software is running, and the medical device security risks involved.
Start with device identity: manufacturer name, model number, serial number, and asset ID. Standard asset data helps teams tie the report to the correct device without delay.
Next, document the software state. That includes the firmware version, OS version, and SBOM reference. The SBOM link helps confirm whether a vulnerable third-party component is part of the device build.
For the vulnerability itself, include the CVE ID and CVSS score. Use CVSS v4.0 and add the full vector string so reviewers can see the safety impact and how the score was calculated.
Clinical context matters. Note whether the flaw affects diagnosis or treatment, could harm a patient, exposes PHI, or could change clinical data. That part can shift how a team handles the issue.
Use U.S. timestamps across every report: MM/DD/YYYY and 12-hour time with time zone, such as 06/27/2026 and 2:30 PM ET. Consistent timestamps support audit trails and remediation tracking. They also make report records easier to match with the asset inventory.
Use these fields as the minimum reporting template.
| Data Category | Required Fields |
|---|---|
| Device Identity | Manufacturer, Model Name/Number, Serial Number, Asset ID |
| Software State | Firmware Version, OS Version, Software Build, SBOM Component Linkage |
| Vulnerability Info | CVE ID, CVSS v4.0 Score (including Safety metric), Vector String |
| Clinical Context | Clinical Use Case, Patient Safety Impact, PHI Exposure Risk |
| Network/Location | IP/MAC Address, Physical Location (Dept/Room), Device Owner |
| Status & Timing | Mitigation Status, Remediation Version, U.S. Date/Time Stamp |
1. Build a Unified IoT Asset and Vulnerability Inventory
You can't report on devices you can't see.
In healthcare, that happens more often than teams expect. Once proper discovery tools are in place, many organizations find they have 15–30% more connected devices than they thought [4]. That blind spot becomes a major issue the moment a new vulnerability appears. Teams need to know which devices are hit, where they are, and who owns them. Without that visibility, every report that follows is built on shaky ground.
The core of this work is a single source of truth inventory. Build it by pulling together data from network discovery tools that use passive deep packet inspection (DPI), your CMMS, NAC platforms, and SIEM/CMDB records. In clinical settings, passive DPI is especially helpful because it identifies devices by watching network traffic, including HL7 and DICOM, without interrupting patient care [4]. Then reconcile what you find across CMMS, CMDB, NAC, and SIEM records so gaps don't stick around.
For each device, keep the inventory centered on continuous synchronization and current device status. That means tracking firmware version, OS build, EOL dates, open ports, encryption, default credentials, physical location, network segment, and ePHI exposure. Each record should also connect to its SBOM. That way, when a CVE is disclosed, you can check right away whether the affected component is part of that device's build.
That kind of current record makes reporting far easier to trace. It also helps teams escalate issues faster and defend remediation timelines with facts instead of guesswork. Just as important, it supports the 72-hour reporting window required by CIRCIA and the 10-day window under FDA 21 CFR Part 806 reporting [2] - deadlines that are almost impossible to hit if your asset records are incomplete.
The table below shows the core inventory fields, where each data point should come from, and how each one supports reporting.
| Inventory Field | Authoritative Source | Reporting Use |
|---|---|---|
| Trade name, model, serial number, firmware version | CMMS, network discovery (DPI) | Device identification in vulnerability reports |
| CVE ID, CVSS v4.0 score, CISA KEV status | SIEM, vulnerability feeds | Severity triage and escalation prioritization |
| IP/MAC address, network segment, physical location | NAC, CMDB | Scope and containment during incident response |
| SBOM component linkage | Manufacturer disclosure, SBOM repository | Rapid impact assessment when a CVE is disclosed |
| EOL/maintenance status, patch history | CMMS, CMDB | Remediation planning and compliance documentation |
This inventory should feed intake and triage, so every new finding maps to a known device before review begins.
2. Standardize IoT Vulnerability Intake and Triage Workflows
Once you have an inventory, the next step is simple: turn new disclosures into reports your team can act on.
That starts with a standard intake process. Pull in new disclosures from automated NVD and CISA feeds. If you skip this step, teams often end up sorting findings one by one and treating disclosure review like paperwork instead of risk management.
Watch these sources closely: NVD, CISA KEV, manufacturer advisories, and healthcare threat-intelligence alerts [3][2]. If a CVE appears in the CISA KEV Catalog, move it to the top of the queue no matter what its base CVSS score says. Why? Because KEV means the flaw is already being used in the wild [3].
Triage also needs a split view: technical severity on one side, clinical risk on the other.
A high CVSS score doesn't automatically mean a device is in danger. The affected code path may be unreachable in your setup. The feature may be turned off. Existing controls may already block the attack path. That's why manufacturer VEX statements matter. When the evidence supports it, use VEX to mark findings as not affected and cut down on noise [3].
Use CVSS v4.0 as your base, then add patient-harm potential and medical device exploitability. From there, map exploitability and patient impact to response timelines.
Use severity bands so teams make the same call in the same situation.
| PSIRT Severity | Triage Window | Required Action |
|---|---|---|
| Critical | 24 hours | Immediate activation; advisory within 48 hours; containment within 72 hours [3] |
| High | 72 hours | Advisory within 5 business days; remediation roadmap within 30 days [3] |
| Medium | 7 days | Remediation in the next scheduled release or within 90 days [3] |
| Low | 30 days | Logging and remediation in the next scheduled release [3] |
Treat every triage call as an auditable quality record. Document each severity decision, each VEX justification, and each escalation path with clear traceability. That record becomes the bridge to clinical-context reporting and incident response.
Once triage is done, the report should spell out the clinical impact and the response path.
3. Document IoT Vulnerabilities With Clinical Context
Documentation should spell out the clinical impact, not just the technical bug. Each IoT vulnerability record needs to show the full path from the exploit to the patient risk: the exploit, the device behavior change, the clinical parameter affected, and the possible patient outcome [2]. That chain is what turns a CVE into an actual risk decision. Put simply, every report has to cover both the flaw itself and what it could do in care settings.
Use CVSS v4.0 first. Then add a plain-English explanation of how the flaw could affect diagnosis or treatment performance, data integrity, or device availability during care delivery and workflow downtime [1][2]. That gives teams a consistent way to document what matters.
| Documentation Element | Required Detail |
|---|---|
| Clinical Context | Primary clinical function and impact on diagnosis or treatment performance [1][2] |
| Impact Pathway | Exploit chain traced to device behavior change and potential patient outcome [2] |
| Risk Assessment | ISO 14971 safety impact and CVSS v4.0 vector string [1] |
| Mitigation Status | Technical compensating controls and clinical workaround plans [2] |
| Remediation History | Patch deployment timeline or justification for any delays [1][2] |
Two regulatory requirements make this level of documentation mandatory. As of February 2, 2026, the FDA's QMSR makes cybersecurity a quality-system requirement. That means vulnerability records must be traceable to ISO 13485 design controls and tied to CAPA records [1][2]. FDA investigators now check cybersecurity documentation during routine QMS audits [1].
It also helps to cross-reference the SBOM so you can identify affected component versions and see where the device is deployed. That detail matters. A device in the ICU may call for faster action than the same model used in outpatient care.
After the clinical record is complete, it becomes the basis for stakeholder communication and escalation.
4. Coordinate Vulnerability Communication Across Internal and External Stakeholders
Once the documentation is done, send the report to each stakeholder fast. Use the clinical impact summary to shape each version. That matters because one IoT vulnerability inside an HDO can hit several teams at once, and each team is looking for a different thing.
The security team wants the technical details: CVE identifiers and CVSS scores. Clinical engineering needs to know if the device must come offline. Executive leadership needs the plain-English version: liability, care continuity, and what kind of risk the organization is carrying.
A RACI matrix helps lock down ownership for each vulnerability type. Without one, IT and biomedical engineering can drift out of sync, especially when a patch needs physical access to a device sitting in a clinical area. And when you write the report, translate the issue into patient-impact language. Focus on what the flaw does to care delivery, not what the code does.
| Stakeholder | Primary Concern | Communication Format |
|---|---|---|
| Security Team (CISO/SOC) | Technical remediation | CVE, CVSS v4.0, IoCs, packet captures, network location |
| Clinical Engineering (Biomed) | Patient safety & device uptime | Device location, maintenance window, safety impact |
| IT Operations | Network dependencies & downtime | EHR integration impact, patching schedule |
| Executive Leadership | Risk, liability & compliance | High-level summary, financial exposure, compliance status |
| Device Manufacturers | Product integrity | Coordinated disclosure packet, reproduction details |
| Regulators (FDA/OCR) | Public safety & compliance | Required filings and safety notices |
| Health-ISAC | Sector-wide threat defense | Anonymized IoCs, TLP-labeled advisories |
Use CVD to push timely manufacturer notice, patches, and validated workarounds. If you're sharing threat intel with groups like Health-ISAC, label it with the Traffic Light Protocol (TLP). For example, use TLP:AMBER when distribution should stay limited, and TLP:GREEN when the information can be shared more broadly.
For shared-component vulnerabilities, line up disclosure timing with CISA and affected vendors. Keep the same tracking ID, CAPA record, and SBOM link across every communication thread.
5. Connect IoT Vulnerability Reporting to Incident Response and Ongoing Risk Management
Once the report is filed, it should turn into the incident record that guides containment, filing, and remediation.
Regulatory Alignment
If a vulnerability crosses the line into a reportable incident or a correction/removal event, send it to the right regulatory owner and start the right reporting clock.
From there, move the case into containment and clinical review.
Clinical Risk Context
Containment calls need clinical review. Don’t isolate a device without it. For life-sustaining devices, use selective controls and document any compensating controls in plain terms. A containment matrix helps here. It should map device criticality and exploit status to the action the team takes.
Reporting Workflow Maturity
Your cross-functional IR team should include Clinical Safety and Regulatory Affairs leads. They need clear ownership of triage, containment, and closure.
Use a three-tier classification so each case lands in the right path:
- Tier 1 (Critical): active exploitation with probable patient safety impact
- Tier 2 (Major): suspected exploitation or high-risk exposure
- Tier 3 (Minor): confirmed vulnerabilities with no current exploitation
That kind of routing keeps teams from treating every issue the same way. And in healthcare, that matters.
Documentation and Traceability
After containment, close the loop with records that show what changed, why it changed, and how the fix was checked. The response record chain should run from the incident ID through root cause analysis, CAPA, design change documentation, validation results, and workaround rationale for any case where immediate patching isn’t feasible.
That record trail supports audit readiness.
| Documentation Category | Required Records |
|---|---|
| Discovery | Incident ID, initial severity, case assignment |
| Remediation | Root Cause Analysis, CAPA record, design change |
| Validation | Verification results, regression and security testing |
| Clinical Context | Patient safety assessment, compensating controls, residual risk |
| Audit Readiness | Evidence retention, training records, program review |
Reference Tables for IoT Vulnerability Reporting
These tables are the day-to-day guide for triage, ownership, and outside disclosure. Use them the same way every time so reports don’t drift, stall, or miss key records.
Severity-to-Action Matrix
This matrix links severity to the action, team, and paperwork that must follow. Once you set severity, you should already know who moves next and what records need to exist.
| Severity | Criteria | Reporting Action | Responsible Team | Required Artifacts |
|---|---|---|---|---|
| Critical | Active exploitation; direct patient safety risk | Escalate immediately | PSIRT Lead, Clinical Safety | Incident Report, Safety Impact Assessment, CAPA Record |
| High | Exploitable; clinically relevant impact | Triage and fix | Vulnerability Analyst, Security Engineer | CVSS Score, SBOM Correlation, Design Change Record |
| Medium | Exploitable; limited clinical impact | Schedule remediation | Security Engineer, Product Manager | Patch Plan, Risk Analysis, Security Advisory |
| Low | Theoretical risk; hard to exploit | Log and monitor | IT, Clinical Engineering | QMS Change Record, Vulnerability Monitoring Plan Entry |
Once severity is assigned, the next step is ownership.
Reporting-Field Ownership
Reports often stall for a simple reason: nobody knows who owns which field. This table fixes that by naming the primary owner, the contributing team, and the handoff record that keeps the trail clear.
| Reporting Field | Primary Owner | Contributing Team | Required Handoff Record |
|---|---|---|---|
| Device Inventory | Clinical Engineering (HTM) | IT / Network Security | Asset Management Database (CMMS) |
| SBOM References | Vulnerability Analyst | Security Engineering | SBOM Revision Record / Incident ID |
| CVEs | Vulnerability Analyst | Threat Intelligence | Triage Report / CVSS Vector String |
| Clinical Use / Context | Clinical Safety Lead | Nursing / Clinical Staff | Clinical Impact Analysis Template |
| Risk Rating | PSIRT Lead | Clinical Safety / Legal | Risk Management File (ISO 14971) for enterprise risk |
| Mitigation Status | Security Engineer | Product Management | CAPA Record / Design Change Notice |
After ownership is clear, send the report through the right outside channel.
External Reporting Channels
Not every disclosure goes to the same place. This table maps the trigger, submission path, and evidence set so the report reaches the right recipient on time.
| Channel | Trigger | Submission Path | Required Data |
|---|---|---|---|
| Manufacturer | Discovery or confirmation of vulnerability | PSIRT intake (email / web form) or automated security questionnaires | CVE, affected version, reproducibility details, PGP-encrypted logs |
| FDA | Correction initiated to reduce health risk, or harm occurred | MDR (21 CFR 803) or 524B disclosure (10-day window) | Health risk assessment, patient harm details, device IDs, field correction plan |
| CISA (CIRCIA) | Covered cyber incident or ransomware payment | CISA Portal (72 hours for incidents / 24 hours for ransomware payments) | Attack vector, impact scope, indicators of compromise |
| ISAC / ISAO | Sector threat sharing | Member portal / TLP-labeled secure communication | IoCs, TTPs, TLP:AMBER or TLP:GREEN advisories |
Use TLP:AMBER for limited distribution and TLP:GREEN for broader sharing.
How Censinet Supports HDO Vulnerability Reporting Workflows
Those reporting fields get much easier to fill out when inventory, assessment, and remediation data sit in one system. These workflows rely on current data that teams can access without digging through scattered records. Censinet RiskOps™ gives HDOs a central place for risk data, vendor assessments, and device documentation.
Censinet RiskOps™ keeps vendor and device risk records together in one place. When new vulnerability details come in, teams can use existing assessment data and device documentation to fill reporting fields faster and keep risk records in sync. Censinet AI™ speeds up intake by summarizing evidence and drafting risk reports from assessment data.
Censinet RiskOps™ also helps HDO teams and vendors work from the same risk record. That makes it easier to coordinate mitigation steps and keep IoT vulnerability reporting in line with shared ownership duties. With one shared record, reporting, mitigation, and ownership stay connected.
For leadership, Censinet RiskOps™ offers cybersecurity benchmarking and a dashboard view of risk across devices, vendors, and open actions. That view helps CISOs and risk program managers track reporting status and remediation progress across devices and vendors.
Conclusion
IoT vulnerability reporting isn't a one-time task. For HDOs, it's a repeatable process. And it matters because device risk can affect patient care, not just IT systems.
These practices work best when they operate as one connected workflow, not as separate tasks. Put simply, they form a single reporting loop: inventory → triage → clinical context → communication → response. That loop is what turns vulnerability reporting into repeatable risk control.
Pressure from compliance keeps growing, and weak reporting can leave patient-safety risk and remediation gaps untreated. For HDOs, the practical focus is consistency: the same report quality, every time. Consistent reporting helps HDOs cut patient risk, meet disclosure duties, and respond faster when new vulnerabilities appear.
FAQs
How can an HDO start if its device inventory is incomplete?
Start with passive monitoring. That means watching network traffic to spot devices without touching them or interrupting sensitive medical equipment. In healthcare settings, that matters a lot. A noisy scan at the wrong time is the last thing anyone wants.
Before you run even light discovery scans, work with biomedical engineering teams to confirm network boundaries. They know which systems are sensitive, which segments need extra care, and where scanning could create problems.
Once devices are identified, sort them by key details such as:
- Manufacturer
- Model
- Firmware
- Configuration
From there, assign risk scores so security teams can decide what needs attention first. Put the highest priority on life-sustaining devices and other high-risk technology, where even a small issue can carry serious patient impact.
When is an IoT vulnerability a reportable incident?
An IoT vulnerability turns into a reportable incident when it creates an uncontrolled risk that can threaten patient safety or disrupt clinical functions.
That’s the line that matters. A flaw on its own may be a security issue. But once it can affect care delivery or put patients at risk, reporting duties kick in.
Manufacturers need to move fast:
- Report risk-to-health correction patches to the FDA within 10 days of starting the action under 21 CFR Part 806
- Report cyber incidents within 72 hours under CIRCIA
- Notify customers within 30 days of finding major uncontrolled risks, even if the final patch still isn’t ready
In plain terms, you can’t wait for the perfect fix before sounding the alarm. If the risk is serious and no longer under control, regulators and customers need to know.
How should HDOs prioritize patient safety risk vs. cyber severity?
HDOs need to weigh technical severity against clinical impact. A risk matrix can help teams sort vulnerabilities based on what could interrupt patient care or expose sensitive data.
Instead of leaning on probability, score each risk by exploitability and clinical criticality. In plain terms: how easy is it to abuse, and what happens in care if it is? That could mean missed therapy, incorrect dosing, or alarm suppression.
If a vulnerability could plausibly lead to patient harm, it should move into the organization’s ISO 14971 safety process.
