Point tools alone are not enough for healthcare anymore. If AI-driven phishing, deepfakes, ransomware, or vendor failures get through, the organizations that do best are the ones that keep care moving, cut downtime, and recover with less damage.
I’d sum up the article like this: healthcare risk now comes from both direct attacks and weak links across vendors, staff workflows, and internal AI use. The answer is not one more tool. It’s a clear resilience model built around risk-based access controls, vendor review, tested downtime plans, staff verification steps, and AI governance with named owners.
Here’s the short version:
- Healthcare is under pressure: hacking made up 79% of major healthcare breaches in 2023.
- Ransomware keeps growing: 67% of healthcare groups reported a ransomware attack in 2024.
- Third-party risk is a big part of the problem: 56% said they had a breach tied to a third party in the last 12 months.
- Downtime is costly: ransomware events can last 17 to 19 days, with about $1.9 million per day in downtime costs.
- Internal AI use adds more risk: about 80% of U.S. hospitals use AI in at least one function, but many still lack clear review and approval steps.
What should you do first?
- Put MFA on remote access, cloud EHRs, and privileged accounts
- Segment clinical, admin, and device networks
- Review third-party vendor risk with proof, not just questionnaires
- Test ransomware, EHR outage, and vendor outage playbooks at least twice a year
- Use call-backs and dual approval for high-risk requests
- Set up an AI governance group with security, privacy, legal, and clinical leaders
- Track a short list of metrics like MTTD, MTTC, uptime, MFA coverage, and vendor findings closed on time
The main idea is simple: if an attack lands, your ability to keep treating patients matters more than having a long list of controls on paper.
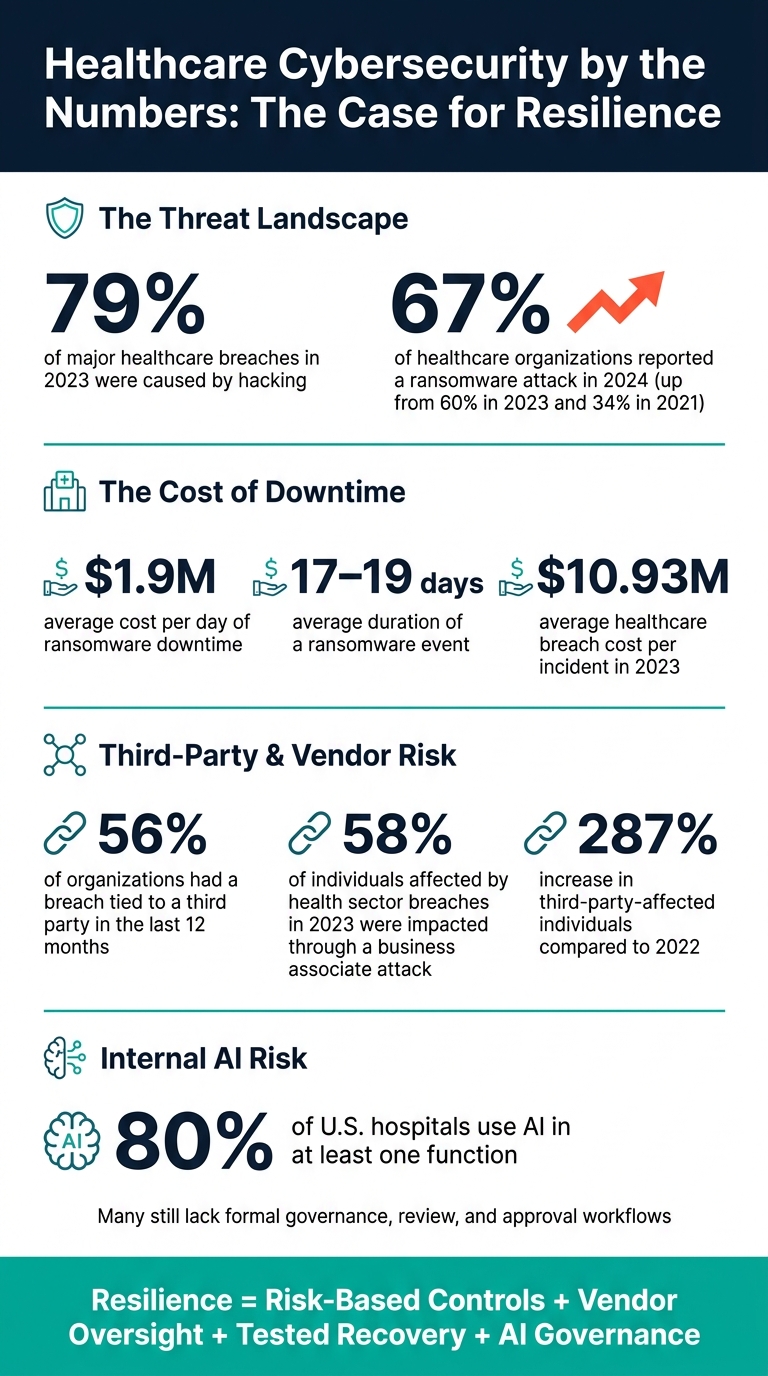
Healthcare Cybersecurity by the Numbers: The Case for Resilience
H-ISAC's Weiss Says Healthcare Cybersecurity Always Comes Back to People
sbb-itb-535baee
Why Traditional Security Programs Fall Behind AI-Driven Attacks
That resilience gap becomes obvious when static controls run into AI-driven attacks. Most healthcare security programs were built for slower, more manual threats. Now AI can automate reconnaissance, phishing, and exploit chaining at a pace that outstrips how fast security teams can review alerts and act. The gap keeps growing: attacks move fast, while response teams are still catching up.
In healthcare, that doesn't just mean IT headaches. It can disrupt care. In 2024, 67% of healthcare organizations reported facing a ransomware attack, up from 60% in 2023 and nearly double the 34% reported in 2021.[4] Those attacks caused an average of nearly 19 days of downtime per incident.[4] Another study found that 41.7% of ransomware attacks led to electronic system downtime, and 4.3% resulted in ambulance diversion.[3]
Where Static Controls Break Down Against Phishing, Deepfakes, and Automated Exploitation
Password-based access leaves healthcare open to phishing and impersonation. AI-assisted phishing can mimic internal writing styles closely enough to trick staff into sharing credentials or approving sensitive requests. Deepfake voice and video tools add another layer of risk. They can imitate executives, clinicians, vendors, or even family members well enough to pressure someone into resetting credentials, approving fake payments, or skipping normal verification steps. A phone approval with no verification trail can turn into an attack path in seconds.
The problem doesn't stop with identity. Delayed patching, flat networks, and uneven logging give automated scanners plenty of room to work. If an organization relies on monthly or quarterly remediation cycles, it's often already behind when fixes finally happen. And without endpoint detection plus centralized logging, security teams may not know whether an alert is harmless noise or the start of a larger compromise. That uncertainty burns time. In healthcare, lost time can affect patient care fast.
How Third-Party Exposure Expands the Healthcare Attack Surface
Healthcare never works alone. EHR integrators, billing processors, imaging platforms, cloud hosts, remote support vendors, and medical device suppliers often have some level of access to clinical or administrative systems. Each connection can become a doorway, not just into one organization, but into every provider tied to that vendor.
The numbers show how serious this has become. In 2023, 58% of the 77.3 million individuals affected by health sector data breaches were impacted through an attack on a business associate. That was a 287% increase in third-party-affected individuals compared to 2022.[5] In a separate finding, 74% of unauthorized access issues in healthcare were linked to third-party vendors.[6] Attackers understand the math here: one vendor can open the door to many providers at once.
The organizations that handle this better don't treat vendor risk like a box-checking task for procurement. They treat it as a patient-care issue. When a key vendor goes down or gets compromised, clinical workflows can stop, revenue cycle operations can stall, and the fallout can hit right away.
What helps is pretty clear:
- Continuous oversight of third-party access
- Contract terms tied to security standards
- Clear mapping of which vendors touch critical workflows
- Risk-based controls and tested recovery plans
That's often the difference between an organization that absorbs the hit and one that gets overwhelmed by a single vendor incident.
The Resilience Model That Helps Healthcare Organizations Stay Ahead of Threats
Once the attack surface is clear, the next job is to lock down the systems and workflows that keep care moving. In practice, resilience comes down to four moves: tiered controls, vendor oversight, tested recovery, and workforce verification.
Risk-Based Controls That Protect Access, Endpoints, and Critical Systems
Not every system carries the same level of risk. Some have a direct effect on patient care. Others hold large amounts of ePHI. That’s why EHR platforms, medication administration systems, and diagnostic imaging networks need tighter protection than scheduling or billing systems. When teams sort systems by impact first, they know where to put controls before anything else.
MFA should go first on remote access, VPN connections, cloud-hosted EHRs, and privileged accounts. Those paths carry the most exposure if an attacker gets in. EDR can spot and isolate ransomware. SIEM ties together identity and system logs. Continuous monitoring helps teams catch odd logins, exports, and access patterns before they turn into something worse.
Network segmentation adds another layer of protection. Keeping clinical, administrative, and medical device networks separate makes a big difference. If someone takes over an email account, that alone shouldn’t open a path to ventilators, infusion pumps, or imaging equipment.
In short, risk-based controls put stronger protections around the systems whose failure would most directly disrupt care or expose large volumes of ePHI.
That same tiered model should carry over to every vendor that touches clinical or financial workflows.
Vendor Risk Management and Continuous Third-Party Oversight
The answer is consistent assessment, evidence validation, and continuous monitoring.
Standardized workflows usually start with structured questionnaires that cover security policies, technical controls, incident response procedures, and regulatory compliance claims. But a questionnaire by itself isn’t enough. Evidence validation means reviewing the actual artifacts: SOC 2 reports, penetration test summaries, BAAs, data flow diagrams that show PHI handling, and disaster recovery documents with recovery time objectives tied to clinical needs.
Take a cloud-hosted PACS vendor. It should be able to show encryption in transit and at rest, role-based access controls, and imaging restoration timelines that fit clinical operations. If a vendor can’t show that clearly, that’s a red flag.
Manual workflows tend to bog teams down. Censinet centralizes questionnaires, evidence sharing, risk scoring, and AI risk oversight in one workflow.
| Dimension | Manual Vendor Risk Process | Censinet RiskOps™-Enabled Workflow |
|---|---|---|
| Assessment speed | Weeks to months per vendor | Days, with automated scoring and standardized questionnaires |
| Consistency | Bespoke, varies by analyst | Standardized control libraries and scoring across all assessments |
| Fourth-party visibility | Limited, often undisclosed | Sub-processors and dependencies mapped within risk inventories |
| Impact on resilience | Reactive, gaps discovered after incidents | Proactive monitoring with continuous posture tracking and audit trails |
Even strong vendor oversight won’t stop every outage. That’s where response speed starts to matter.
Incident Response, Downtime Readiness, and Workforce Verification
Incident response readiness shapes how much damage happens when something slips through.
Resilient healthcare organizations build scenario-based playbooks for ransomware, account compromise, and vendor outages. Then they test them. Run at least two tabletop exercises each year, and include ransomware, EHR outage, and vendor outage scenarios. Downtime drills also matter because clinical staff need practice with paper-based workflows, pre-printed order sets, and manual verification steps for medication ordering, documentation, and lab results.
Break-glass access gives authorized clinicians emergency access to critical systems during outages, and each use should be logged and reviewed after the fact so emergency access doesn’t turn into an open gap. [8]
Workforce verification covers the human side. For high-risk actions like changing a vendor’s ACH information, granting elevated system access, or approving large-dollar payments, require call-back verification through a trusted channel before approval. Dual-control approval workflows add one more check so no single person can approve a sensitive transaction alone.
Deepfake threats make this even more important. Staff should treat urgent requests from executives or clinicians as possible impersonation attempts. That means getting secondary confirmation through known channels instead of acting on a phone call or video alone. Training should show, in concrete terms, how AI can mimic voices, faces, and writing styles. [7]
A few identity hygiene steps help close the loop:
- Quarterly access reviews
- Immediate account disablement on termination
- Automatic expiration for contractor accounts
These steps help stop compromised credentials from turning into long-term footholds.
The same verification discipline should apply to internal AI tools, model approvals, and PHI use.
How AI Governance Turns Internal AI Use Into a Managed Risk
The same verification standard now has to apply to internal AI use too. Around 80% of U.S. hospitals use AI in at least one clinical or operational function, yet many organizations still have governance that lags behind that use.[9] That leaves patient data, clinical workflows, and admin systems exposed.
When governance is missing, the problems are pretty direct. Staff may paste PHI into unapproved tools. Vendors may mishandle patient data. Clinical AI may shape care decisions without a human checking the output first. That goes beyond a compliance issue. Poorly managed internal AI can trigger the same kind of resilience problems seen in outside attacks: data leaks, bad decisions, and disrupted workflows.
AI Governance Roles, Policies, and Review Workflows
A formal AI governance committee is where this starts. It should include the CISO, IT operations, compliance and privacy officers, legal, clinical leadership such as the CMO, CMIO, or CNIO, and enterprise risk management. Each group needs a clear job. Security handles data flows and access controls. Compliance covers HIPAA and state privacy rules. Clinical leaders review safety and bias. Legal reviews contracts and liability.
This group should meet monthly and use standard intake forms plus a risk-scoring method so each AI proposal goes through the same review process.
The committee also needs a living AI use policy.[11][12] That policy should spell out:
- Which data types can go into which tools
- When clinical AI needs human review before anyone acts on its output
- How vendors must show compliance, including SOC 2, HITRUST, and BAAs as part of a strategy to effectively manage third-party risk
- What staff can and cannot enter into consumer or unmanaged AI tools
High-risk use cases, especially anything tied to diagnosis, triage, or treatment, should require committee approval and human review. Lower-risk admin automation can move through a faster review path, but it still needs an audit trail. That link matters because strong AI governance supports patient safety, uptime, and compliance - the same outcomes resilience is meant to protect.
At scale, this only works with one shared workflow for intake, review, and approval.
Using Centralized Risk Operations to Maintain AI Oversight
Trying to manage AI governance across many departments with email threads and spreadsheets falls apart fast. Censinet AI within Censinet RiskOps™ puts AI policies, risks, and tasks in one place and sends findings to the right owner. If a privacy gap shows up during an AI vendor assessment, it goes straight to the Privacy Officer with a due date. If a security control is missing, it goes to the CISO. Every action is logged, which creates an audit trail for OCR reviews and internal audits.
Censinet AI can draft policy language, summarize vendor documents, and flag risk patterns while humans keep final approval.[10] That gives healthcare leaders one AI risk dashboard with a real-time view of approved tools, open findings, remediation progress, and regulatory alignment across the enterprise.
Centralized workflows help keep each governance step consistent.
| Governance Function | Accountable Role | Resilience Outcome |
|---|---|---|
| AI Use Approval | AI Governance Committee | Alignment with safety, ethics, and organizational goals |
| Data Leakage Prevention | Privacy & Security Officers | Prevention of data breaches and HIPAA violations |
| AI Vendor Review | IT & Procurement | Reduced risk from third-party AI tools and sub-processors |
| Clinical Safety Review | Chief Medical Officer (CMO) | Mitigation of AI bias and improved patient outcomes |
| Threat Detection | CISO / SOC Team | Early detection of unauthorized activity and AI-related incidents |
That same discipline - clear roles, documented approvals, and continuous monitoring - is what separates organizations that manage AI risk from those that only find it after a breach.
Conclusion: The Healthcare Outcomes That Justify Resilience Investment
The case for resilience comes down to money and day-to-day performance. Healthcare breach costs hit $10.93 million per incident in 2023 and about $7.42 million in 2025.[13][14][2][1] Resilience does not stop every attack. What it does is shrink the blast radius.
When phishing, deepfakes, or automated exploitation slip through, speed changes the outcome. Early detection, fast containment, and limited exfiltration can cut losses from more than $10 million to about $1,500,000 to $2,500,000. And the gap gets even bigger when patient care is disrupted. Ransomware downtime costs U.S. healthcare organizations about $1.9 million per day, and the average event lasts 17 to 18 days.[15][16] Teams with tested downtime procedures and rehearsed response plans can reduce that window in a meaningful way.
The same logic applies to compliance. Organizations with a clear audit trail of decisions, fixes, and governance actions are in a much better spot when pressure hits. They can recover faster, document actions more cleanly, and face less enforcement risk if OCR reviews the incident. That is why resilience should be tracked with the same seriousness leaders bring to revenue and patient safety.
The organizations staying ahead of AI-driven threats are not guessing. They measure, rehearse, and keep getting better. Those results should appear in a small set of core metrics.
Key Resilience Metrics Healthcare Leaders Should Track
| Metric | What It Measures | Why It Matters |
|---|---|---|
| EHR and critical system uptime | Percentage availability of EHR, PACS, pharmacy, and scheduling systems | Tied directly to patient throughput, revenue, and continuity of care |
| Mean Time to Detect (MTTD) | Average time from breach initiation to detection | Breaches often go unnoticed for about 212 days,[2][17] so lower MTTD means fewer exposed records and less regulatory risk |
| Mean Time to Contain (MTTC) | Average time from detection to containment | Faster containment cuts downtime costs and limits lateral movement |
| High-risk vendor findings remediated | Number and percentage of critical third-party risk findings closed within target timeframes | Third-party attacks accounted for 58% of individuals affected by healthcare breaches in 2023.[5][18] |
| Privileged accounts protected by MFA | Percentage of privileged and remote-access accounts with MFA enforced | Lowers the success rate of AI-driven phishing and credential attacks |
| Breach cost and records exposed | Records affected per incident; direct losses in dollars | Turns technical results into financial and regulatory terms boards and executives can use |
Track these metrics on a steady basis, and resilience stops being a vague goal. It becomes something leaders can see, test, and improve before risk shows up too late.
FAQs
What makes healthcare resilience different from cybersecurity alone?
Healthcare resilience goes beyond cybersecurity because it puts care continuity first, not just defense.
Cybersecurity is about protecting data and blocking unauthorized access. Resilience is broader. It helps healthcare groups keep working through disruptions like cyber incidents, vendor outages, device failures, and supply chain shortages.
It pulls cyber, clinical, vendor, and operational teams into one response model. The aim isn’t just to stop attacks. It’s to cut downtime and reduce patient harm when systems break.
How should hospitals prioritize resilience investments first?
Start with an enterprise-wide risk assessment that ranks systems based on their impact on patient care and the fallout from downtime.
Leaders should also map vendor dependencies to clinical and business workflows so they can spot single points of failure. When teams frame decisions around risk reduction instead of old-school ROI, it becomes much easier to justify spending on tools and processes that protect continuity, detect threats in real time, and automate risk management.
Who should own AI governance in a healthcare organization?
AI governance should be an enterprise-wide program, not something tucked away as an IT-only project. It touches clinical care and day-to-day operations, so ownership needs to be shared across the CMIO, compliance, data science, legal, and IT security.
Oversight committees can help set clear decision rights, accountability, and escalation paths. And each AI tool should have a named owner responsible for monitoring, access limits, and regular revalidation.
