Rural providers are not treating AI like a lab project. They are using it to cut charting time, protect cash flow, tighten security, and help small teams do more with less.
If I had to sum up the article in a few lines, it would be this:
- Start with pain points, not hype
- Pick one narrow workflow first
- Track a few hard metrics for 60 to 90 days
- Keep human review in place
- Check third-party AI risk before any contract is signed
The article shows a clear pattern. Rural hospitals face thin margins, staff shortages, aging systems, and long patient travel times. So AI only makes the list when it can fix work that is slow, manual, or draining staff time right now.
Here’s where leaders are looking first:
- Ambient documentation to cut after-hours note work
- Revenue cycle tasks to reduce manual billing effort and denial drag
- Imaging support to ease bottlenecks
- Patient access tools for scheduling and intake flow
- Cybersecurity monitoring to help small IT teams keep up
But the article also makes one point very clear: every AI tool adds risk. That includes PHI exposure, vendor risk, hidden fourth-party risk, and shadow AI. And with AI-related cyberattacks up 300%, rural teams cannot skip governance just because they are small.
A fast way to think about the article is this:
| Focus area | Why it comes first | Main watch-out |
|---|---|---|
| Documentation | Less note burden | PHI and human review |
| Revenue cycle | Better cash flow | System fit and oversight |
| Imaging | Less delay | High data exposure |
| Patient access | Less admin work | Vendor and workflow control |
| Security | Helps lean IT teams | Tool sprawl |
My takeaway: rural AI works best when leaders stay narrow, measure results, keep a simple inventory of tools and data flows, and make vendor review part of procurement from day one.
That is the article’s core message in plain English: small pilot, clear metrics, tight oversight, then scale only if the numbers support it.
H-ISAC's Weiss Says Healthcare Cybersecurity Always Comes Back to People
sbb-itb-535baee
Where rural health leaders are focusing AI first
Rural health leaders are starting with a small set of AI use cases that offer clear ROI and don't take a massive overhaul to put in place. The pattern is pretty simple: go after work that eats up staff time, slows patients down, or piles more pressure on already thin teams.
That shows up most often in documentation, revenue cycle, imaging, patient access, and security workflows.
Ambient documentation and revenue cycle automation
Ambient clinical documentation is getting early attention because it goes straight at one of the biggest pain points in care delivery: note burden. Healthcare AI is projected to cut clinician documentation time by about 20%[3]. In rural settings, that matters even more, since clinicians often wear multiple hats during the day.
Revenue cycle work fits the same logic. A lot of it is repetitive, manual, and time-consuming. Automating parts of that process can ease pressure on back-office teams and help work move faster without adding headcount.
Imaging support and patient access workflows
Imaging support and patient access tools are also high on the list. Why? Because they can ease bottlenecks without forcing major workflow change.
Across both areas, the goal is the same:
- Fewer bottlenecks
- Less manual coordination
- Faster throughput
AI for cybersecurity monitoring in small environments
AI is also showing up in cybersecurity, especially in third-party risk management. For small teams, automating vendor follow-up can save a lot of time and cut down on missed steps.
"The ability to have vendors already in the catalog and automate follow-ups has been super important. We now have a system that enforces accountability and ensures vendor compliance before contracts are signed." - Brian Sterud, CIO/CISO, Faith Regional Health Services[1]
That same approach - automate repeatable work and keep human review for judgment calls - also shapes how rural leaders think about risk. These early use cases look attractive for a reason, but they also widen the risk surface leaders have to manage next.
What makes AI risky in rural healthcare settings
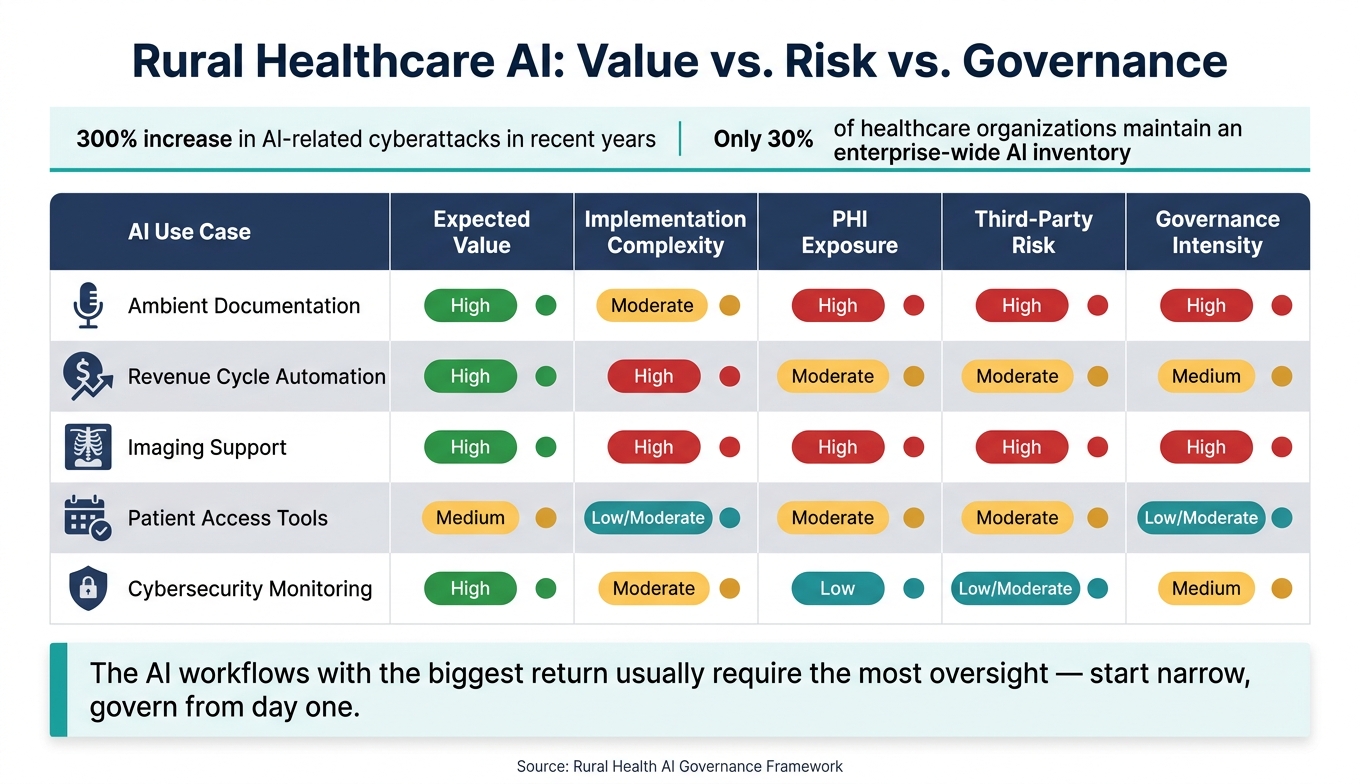
Rural Healthcare AI Use Cases: Value, Risk & Governance at a Glance
The same AI tools that save time on charting, billing, and patient access can also open up new risk. In rural hospitals, that tradeoff hits harder. Teams are often small, vendor visibility can be limited, and response time is often slower when something breaks. So while the upside is clear, the attack surface grows at the same time. AI-related cyberattacks have increased by 300% in recent years [4].
Cybersecurity, PHI handling, and hidden attack surface
Each AI tool connected to an EHR, imaging platform, or patient access workflow creates another possible entry point. Ambient scribes process full clinical audio. Phone AI agents work with scheduling and triage data. In many cases, those tools depend on outside cloud systems, which means PHI passes through platforms the rural provider doesn't directly control.
That matters. If data isn't protected with end-to-end 256-bit AES encryption and tight access controls, it can be exposed in transit or at rest [4].
There's another layer too: fourth-party risk. A hospital may vet its vendor, but what about that vendor's cloud provider or AI model host? If one of those outside partners has a security gap, the rural hospital can still end up dealing with the fallout [1].
"One of the biggest takeaways has been clearly defining risk acceptance. In the past, stakeholders didn't always realize that by not funding security initiatives, they were implicitly accepting risk." - Brian Sterud, CIO and CISO, Faith Regional Health Services [1]
Governance, compliance, and human oversight requirements
Rural providers need a simple AI inventory. Nothing fancy. Just a clear record of every tool in use, the data it touches, and who owns it. Without that, it's hard to know what's live, much less respond when something goes wrong. This gets even harder when staff start using tools outside formal procurement. Shadow AI is a real pattern in resource-constrained settings [4].
Compliance is tightening too. HHS is shifting previously "addressable" HIPAA controls into mandatory requirements, including annual asset inventories and network maps that show AI data flows [3]. For rural leaders with lean teams, the NIST AI Risk Management Framework offers a practical way to review model behavior, bias, and oversight needs. Even so, fewer than 60% of organizations have finished a formal AI risk assessment [4].
Comparison table: rural AI use cases by value, complexity, and risk
The pattern is pretty straightforward: the AI workflows with the biggest return usually need the most oversight.
| AI Use Case | Expected Value | Implementation Complexity | PHI Exposure | Third-Party Risk | Governance Intensity |
|---|---|---|---|---|---|
| Ambient Documentation | High | Moderate | High | High | High |
| Revenue Cycle Automation | High | High | Moderate | Moderate | Medium |
| Imaging Support | High | High | High | High | High |
| Patient Access Tools | Medium | Low/Moderate | Moderate | Moderate | Low/Moderate |
| Cybersecurity Monitoring | High | Moderate | Low | Low/Moderate | Medium |
That's why many rural leaders put guardrails in place first, then think about scale.
How rural organizations are putting guardrails around AI deployment
Once leaders pick a high-value use case, the next move is simple: test it in a small setting and put controls around it from day one.
Start narrow: phased pilots with clear success criteria
Start with one workflow, one department, and three to four metrics.
For ambient documentation, one of the highest-value workflows already identified, begin with a small group of clinicians in a single clinic. Track average charting time per visit, note completion rate by end of day, and how often notes are edited before signing. Run the pilot for 60 to 90 days, then make a formal call: expand, adjust, or stop. If clinicians rarely change AI-generated notes, don’t assume the tool is perfect. Treat that as a sign to reinforce human review.
For revenue cycle AI, begin with a tighter use case like automated claim status checks or denial categorization. Measure manual touches per claim and days in accounts receivable before and after the pilot. If those numbers move in the right direction, that gives the team a case for broader rollout.
If a pilot shows value, the next issue is whether the organization can govern it without slowing everyone down.
Build a small governance process for small teams
Rural organizations don’t need a big committee. They need a small, cross-functional group that meets monthly and stays focused on three questions:
- What new AI tools are being proposed?
- What risks and controls are documented?
- What do the current metrics show?
That group should include a clinical leader, an IT or security lead, a compliance or privacy officer, and an operations or finance leader. The National Rural Health Association also recommends adding patient advocates, providers, and IT specialists. [2]
Start with a few basic tools: an AI inventory, risk register, approvals log, data-flow map, and fallback plan. Each one helps answer the same problems flagged earlier, including PHI exposure, shadow AI, and fourth-party risk. A shared spreadsheet with clear ownership and quarterly updates is enough to get started.
A benchmarking study cited by Censinet found that 70% of healthcare organizations have AI governance committees, but only 30% maintain an enterprise-wide AI inventory. [5]
That process matters most when vendor review follows the same standard every single time.
Standardize third-party AI due diligence with Censinet
Ad hoc vendor reviews fall apart fast once AI tools start touching PHI across several workflows. Rural organizations need a repeatable process that small teams can keep up with.
Faith Regional Health Services in northeast Nebraska made that move under CIO and CISO Brian Sterud. The team shifted to standardized assessments that require vendors to complete a risk review before any contract is signed.
"The ability to have vendors already in the catalog and automate follow-ups has been super important. We now have a system that enforces accountability and ensures vendor compliance before contracts are signed." - Brian Sterud, CIO and CISO, Faith Regional Health Services [1]
Use Censinet RiskOps to standardize third-party risk management for AI vendors, document fourth-party exposure, and route findings for human review before contract signature.
Conclusion: The rural AI approach is selective, risk-aware, and focused on operations
Rural leaders are using AI with care. They’re not rolling it out everywhere. They’re choosing the places where it can help day-to-day operations, work for small teams, and stay under clear oversight. So the next move isn’t broader testing. It’s tighter execution.
The practical path is simple: start small, keep governance lean, and scale only when the results are clear.
What leaders should prioritize next
Start with one or two high-value administrative workflows, then bring in AI through a narrow pilot before scaling. Put risk review into procurement policy before any contract is signed, so vendors must pass security and compliance checks up front.
Keep governance light but steady, and make sure decisions, risks, and follow-up actions are tracked. For rural organizations, consistency matters more than complexity. That’s what keeps AI useful instead of turning into a source of risk.
Rural AI works best when leaders start small, govern lightly, and require vendor accountability from the start.
FAQs
How should a rural hospital choose its first AI pilot?
Start by making a simple inventory of every AI tool already in use, and assign one owner to each tool. After that, rank them based on clinical impact, data sensitivity, and how tightly they connect to day-to-day workflows.
Keep the first wave focused on low-risk use cases, like administrative support or drug-interaction checks. Stay away from high-risk areas at the start, such as diagnostic support or autonomous decision-making.
Before anything goes live, test it locally on 20 to 50 cases and write down clear pause rules in advance.
What metrics best show whether an AI tool is worth scaling?
Focus on metrics that show clear clinical, operational, or financial impact in high-friction, repetitive rural workflows. You want proof you can measure: less time spent on documentation, less admin busywork, and better reimbursement.
For clinical tools, keep a close eye on error rates, clinician override frequency, performance across patient subgroups, and model drift over time. Those metrics help confirm the tool remains safe, unbiased, and effective.
What AI governance steps are essential for small rural teams?
For small rural teams, AI governance works best as a standardized, lifecycle-based process - not a one-and-done checklist.
Start with a plain, up-to-date inventory of every AI tool in use. Each tool should have one clear owner: a clinical, business, or technical lead who’s accountable for it.
Then sort tools into risk tiers based on factors like:
- Clinical impact
- PHI handling
- EHR integration
For high-risk tools, set stricter rules from the start. That means human review, strict BAAs, pre-defined stop rules, and ongoing monitoring for model drift and vendor changes.
Related Blog Posts
- Clinical Intelligence: Using AI to Improve Patient Care While Managing Risk
- The Augmented Physician: How AI is Transforming Clinical Practice and What Healthcare Leaders Must Know
- Guardrails Without Gridlock: Enabling Safe AI Innovation in Healthcare
- The AI-Ready Organization: Cultural and Technical Prerequisites for Success
