AI in healthcare can fail in a clear sequence: attackers find the system, tamper with data or inputs, push the model into bad actions, and then harm care, billing, privacy, or uptime.
If I had to boil this article down, I’d say this: map every AI workflow, check where data enters, limit what AI tools can do, and watch outputs before they affect patients or records. That matters because the risks are not small. The article cites 94.4% prompt injection success in one study of medical LLMs, plus 993 vulnerabilities across 966 ML-enabled medical devices.
Here’s the short version of what you need to know:
- The AI kill chain is a step-by-step attack path
- In healthcare, the main stages are:
- Reconnaissance
- Data poisoning
- Model manipulation and prompt abuse
- Privilege escalation
- Workflow impact
- The main systems at risk include:
- Imaging and pathology models
- Clinical LLMs and charting tools
- AI-enabled medical devices
- Revenue cycle and coding tools
- Third-party AI services
- The biggest outcomes are:
- Patient harm
- PHI exposure
- Downtime
- Billing mistakes
- Care delays
- The main checks are:
- Data lineage review
- Input filtering
- Output review
- Access limits
- Vendor review
- Incident playbooks
A few facts stand out. The article notes that more than 80% of reported events in one medical device study were linked to data acquisition problems. It also points to 160 public exploits tied to device weaknesses that could hit hospitals or patients.
That’s the core idea: if you treat AI risk as a chain instead of a single event, you can spot weak points sooner and assign owners before a bad output turns into a patient, privacy, or business problem.
The Core Stages of the AI Kill Chain in Healthcare
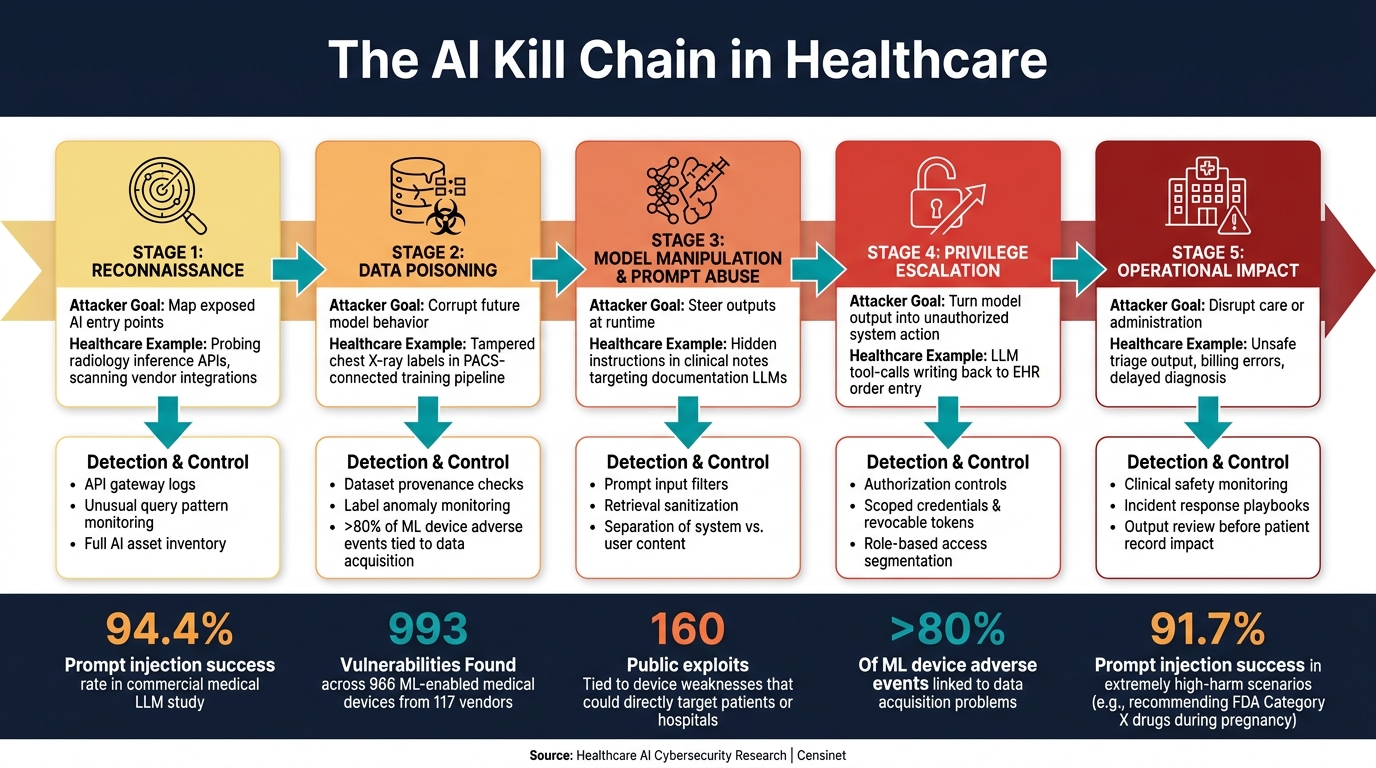
The AI Kill Chain in Healthcare: 5 Attack Stages & Key Controls
The stages below show how attackers move through healthcare AI systems - and where security and clinical teams have a chance to stop them.
| Stage | Attacker Objective | Healthcare Example | Detection Point |
|---|---|---|---|
| Reconnaissance | Map exposed AI entry points | Probing a radiology inference API or reviewing public documentation, model cards, and exposed integrations | API gateway logs, unusual query patterns |
| Data Poisoning | Corrupt future model behavior | Tampered chest X-ray labels in a PACS-connected training pipeline | Dataset provenance checks, label anomaly monitoring |
| Model Manipulation & Prompt Abuse | Steer outputs at runtime | Hidden instructions in clinical notes targeting a documentation LLM | Prompt filters, retrieval sanitization |
| Privilege Escalation | Turn model output into unauthorized access or action | LLM tool-calls that write back to EHR order entry | Authorization controls, action approval workflows |
| Operational Impact | Disrupt care or administration | Unsafe triage output, billing errors, delayed diagnosis | Clinical safety monitoring, incident response |
Reconnaissance and Data Poisoning
Attackers usually don’t begin by going straight at the model. They first look for openings. In healthcare, that often means scanning exposed APIs, vendor integrations, imaging workflows, and clinical LLMs to see what’s reachable and how systems connect.
After that mapping work, data poisoning becomes one of the most dangerous paths. Poisoned fine-tuning data can push medical LLMs toward unsafe drug or imaging recommendations while still passing normal tests.[4][6] That’s what makes this stage so tricky: the model may look fine on the surface.
In imaging pipelines, the risk gets even sharper. If an attacker gets into a PACS repository or a cloud storage bucket, they can quietly alter labeled images so a radiology model learns the wrong pattern. A model might start missing early-stage disease, and that shift may stay hidden until it shows up in patient care.
Once attackers understand the environment, poisoned data can shape model behavior before deployment.
Model Manipulation, Prompt Abuse, and Privilege Escalation
After deployment, the playbook changes. Attackers move from training-time interference to runtime manipulation.
Adversarial examples - inputs with tiny, often hard-to-notice perturbations - can cause imaging AI to misclassify cancerous lesions as benign across chest X-ray, dermoscopy, fundoscopy, and mammography workflows.[1][2][7] A small change in the input can lead to a very different output. That’s a bad trade in any setting, but in clinical care, it can carry obvious patient risk.
Backdoor attacks are even more deceptive. The model behaves normally on almost everything, then flips to attacker-controlled output when a trigger appears. That trigger could be a certain pixel arrangement in a CT series or a keyword phrase inside a clinical prompt.
Prompt injection has the same “looks harmless until it isn’t” feel. It can hide in imaging data, zero-width characters, Unicode, whitespace, metadata, or other runtime inputs.[5] So the input may not look suspicious to a person skimming it, yet it can still steer the model.
The stakes jump when these models connect to EHRs, scheduling tools, or device controllers through tool-calling interfaces. At that point, prompt injection is no longer just about bad answers on a screen. It can drive system behavior.
When tool-calling is enabled, prompt abuse can turn into unauthorized system action.
Operational Impact on Clinical and Administrative Workflows
These stages matter because the end result isn’t abstract. The harm can hit clinical care, finances, and compliance all at once.
Patient safety is the clearest risk. Unsafe triage recommendations, missed diagnoses, or altered treatment suggestions can reach clinicians without obvious warning signs. That’s the hard part: the output may look normal enough to pass at a glance.
The damage also spreads into administrative work. Documentation assistants manipulated through poisoned templates can systematically under-code diagnoses, which affects reimbursement, malpractice exposure, and care continuity. A small change in documentation logic can snowball fast.
In connected device settings, AI systems that depend on tampered telemetry from infusion pumps or monitoring equipment can add noise to the workflow by creating alert fatigue - or, worse, fail to flag deterioration events. PHI exposure through model inversion or membership inference attacks adds privacy and compliance risk on top of the clinical impact.
The next section shows where to detect these attacks and which controls break the chain earliest.
sbb-itb-535baee
Detection Points and Controls Across the Kill Chain
Each stage in the AI kill chain has a matching control point. And the earlier you catch trouble, the less damage it can do.
Threat Modeling, Asset Mapping, and Data Integrity Controls
Start with a full AI asset inventory. That means every AI asset: endpoints, training data, vector stores, prompt caches, EHR links, device connections, and vendors. Each one should have a clear owner and a main threat tied to it.
Once that inventory is in place, threat modeling can zero in on the highest-risk flows, especially anywhere training data enters the pipeline. A study of adverse events in ML-enabled medical devices found that more than 80% of reported events were tied to data acquisition problems.[10] That puts data integrity at the top of the control list.
Every model update, retraining event, or new vendor integration should go through a production review. That review should verify lineage, retest performance, and approve vendor changes. In plain terms, you want to know where the data came from, whether the model still performs as expected, and whether a new third party introduces risk. That cuts the odds of altered orders, missed findings, or PHI leakage.
Once data and integrations are under control, the focus shifts to runtime behavior: abuse, misuse, and drift.
Inference Monitoring, Privacy Defenses, and Prompt Safeguards
Watch for query spikes, unexpected tool calls, and odd outputs before harm reaches a clinician or the patient record.
Adversarial testing should be part of every pre-deployment review for safety-critical models. A recent adversarial ML analysis of 966 ML-enabled medical devices from 117 vendors found 993 vulnerabilities, with 160 having publicly available exploits that could directly target patients or hospitals.[10] That's not just a lab problem. It's the kind of issue that can hit production.
For LLM-based clinical workflows, a few controls matter most:
- Input validation
- Strict separation of system instructions from user-supplied content
- Response validation before output reaches a clinician
Privacy audits should also test for PHI leakage through LLM outputs and logs.[9]
Those controls get stronger when access and vendor dependencies are locked down too.
Least Privilege, AI Supply Chain Security, and Vendor Assessment with Censinet
Apply least privilege to every AI integration: scoped credentials, role-based access, segmented permissions, and revocable tokens. The idea is simple. If one AI component gets breached, it should not be able to reach EHR order entry, device controls, or admin functions it was never supposed to touch.
Patching, dependency review, change validation, and post-update reassessment should be standard AI supply-chain controls. FDA guidance for AI-enabled medical devices explicitly calls out AI-specific cyber threats - data poisoning, model inversion, model evasion, data leakage, bias manipulation, and performance drift - and requires mitigation and lifecycle management plans.[11][3]
This is where Censinet RiskOps™ helps in a direct way. The platform centralizes AI-related policies, risks, and tasks while streamlining third-party AI risk assessments and remediation tracking. Censinet AI™ speeds assessments by summarizing vendor evidence, capturing integration details, and drafting risk reports for human review.[8] The upside is pretty clear: faster and more consistent third-party review, while keeping human approval in place.
The next layer is governance: policies, ownership, and incident response.
Governance and Risk Management for AI in Healthcare
Governance turns kill-chain controls into action with clear ownership. Once you know the attack path, governance answers the practical questions: Who can step in? When do they step in? And how fast?
AI Governance Committees, Policies, and Incident Playbooks
A healthcare AI governance committee needs formal authority. In plain English, it needs the power to approve, pause, or require fixes for any AI system across the full lifecycle, from procurement to retirement. Core members should include leaders from clinical, IT, compliance, privacy, security, operations, and ethics. If there’s no ethics or health equity voice at the table, bias risks are much easier to overlook.
The committee should stay tied to kill-chain risk, especially data poisoning, prompt abuse, and privilege escalation. The policy framework should cover four areas:
- Data integrity and provenance policies should define approved data sources, labeling rules, and controls to block unauthorized changes.
- Model lifecycle policies should require documented architecture, training data, validation results, and change-management steps for any retraining event.
- Privacy and security policies should address PHI handling, access controls, and safeguards against prompt abuse or exfiltration.
- Vendor and third-party policies should set due-diligence requirements and contract standards for AI suppliers.
Those policies should connect to version-controlled review forms and risk checklists. Otherwise, they can sit on a shelf and do nothing.
Policies matter only if they lead to a clear response path. Each playbook should line up with the kill-chain stage it is meant to stop:
- Data poisoning: If there are signs of unusual access or training-data tampering, isolate the dataset, verify source lineage, review logs, and notify data governance and security leads.
- Prompt abuse or model drift: If outputs show signs of adversarial prompting or unexpected drift, suspend the affected features, review prompt logs, compare behavior to approved baselines, and notify clinical leaders to assess patient impact.
- Privilege escalation: If unauthorized model changes or admin actions take place, revoke credentials, run forensic analysis, and review role-based access controls.
The Health Sector Coordinating Council's 2026 AI cybersecurity guidance includes a healthcare AI incident response playbook framework built around clinical environments.[15][16]
Third-Party AI Governance and Continuous Oversight with Censinet
For vendor AI, governance has to move beyond a one-time review. It needs continuous oversight. Vendor AI stretches the kill chain across training data, prompts, access, and retraining, while the organization does not control the full stack.
Censinet RiskOps™ and Censinet AI™ support continuous oversight of vendor AI after the first assessment, while keeping governance workflows in one place and preserving human approval.
Each AI system should have a named clinical owner and a named technical owner. Those people are responsible for monitoring performance and escalating issues when something looks off. AI-related checks should also be built into standard change-management work, including EMR updates, new device integrations, and vendor patches, so AI impact gets reviewed alongside other IT governance decisions. For regulated medical-device AI, the FDA's total product lifecycle framework reinforces that deployment is only the start of monitoring.[12][13][3][14]
Conclusion: Turning the AI Kill Chain Into an Actionable Healthcare Defense Model
Now that the attack stages and controls are clear, the next move is to put them to work. Use the AI kill chain to map attacks from reconnaissance and poisoning to manipulation, privilege escalation, and workflow impact. That gives security, IT, and compliance teams a shared framework for linking controls directly to patient safety.
The risk here isn’t abstract. It shows up in hard numbers. In one study of commercial medical LLMs, prompt injection attacks succeeded in 94.4% of trials overall, including 91.7% of extremely high-harm scenarios such as recommending FDA Category X drugs during pregnancy.[17]
A good place to start is simple: build an inventory of every AI-enabled workflow, map each one to the kill-chain stages, and fix the highest-risk gaps first. Put patient safety at the top of the list, then business continuity. That inventory should shape governance decisions, not sit in a folder as paperwork.
Oversight also needs a steady rhythm. Governance committees, clear policies, and incident playbooks help keep review active instead of one-and-done. For third-party AI risk management, Censinet RiskOps™ and Censinet AI™ can centralize AI risk reviews, send findings to the right owners, and keep human review in the loop.
Treat the AI kill chain as an operating model, not a checklist. That mindset helps teams spot threats earlier, respond with less delay, and keep AI aligned with clinical safety.
FAQs
How is the AI kill chain different from traditional cyberattacks in healthcare?
The AI kill chain differs from standard healthcare cyberattacks in one big way: it goes after the system’s intelligence and decision-making logic, not just the pipes and servers underneath it.
Most healthcare attacks aim to steal data, lock people out, or shut systems down. AI-focused attacks work differently. Tactics like data poisoning, adversarial inputs, and prompt injection try to bend how the model learns, interprets information, or responds.
That’s what makes this so tricky. The system may look like it’s working just fine on the surface. But behind the scenes, it can start producing flawed, malicious, or biased outputs - and those outputs can shape clinical decisions and patient outcomes.
Which healthcare AI systems are most at risk first?
In healthcare, the first systems at risk are the ones AI can touch right away: EHRs, clinical imaging systems, connected medical devices, and cloud-based AI tools.
EHRs tend to be the main target. Why? They store sensitive patient data and often open the door to broad operational access across the organization. If someone gets in there, the damage can spread fast.
There’s also the issue of Shadow AI. These are tools teams start using without formal IT review. They may seem harmless at first, but they can create immediate gaps in security and oversight.
On top of that, high-risk workflows like triage and diagnostics are exposed too. Those areas can be manipulated, and they’re also at risk from data poisoning, which can distort outputs and affect care decisions.
What should a hospital do first to reduce AI risk?
Start with a full inventory of every AI system your organization uses. For each tool, note what it does, what data it touches, and where it shows up in clinical and administrative workflows.
That means documenting things like:
- the tool’s role
- the data it processes
- whether it handles protected health information
- whether it affects clinical decisions
- who uses it and in which workflow
At the same time, put a clear AI use policy in place, along with a formal intake process. Any tool that accesses protected health information or has a role in clinical decision-making should go through review before deployment.
This gives you a practical way to spot shadow AI, rank risk, and support governance over time.
