2026 is the year AI governance in healthcare stops being optional. I see three forces hitting at once: new federal and state rules, more use of AI in care and payment decisions, and higher risk from vendors, audits, and patient harm.
If I had to sum up the article in plain English, it’s this:
- AI use grew faster than oversight
- Regulators now want proof, not broad policy statements
- State laws are making one-size-fits-all oversight harder
- Patient safety, privacy, billing, and vendor risk are now tied to AI use
- Health systems need clear ownership, written rules, audit logs, staff training, and post-launch review
- Teams also need one place to track AI tools, vendor reviews, exceptions, and human overrides
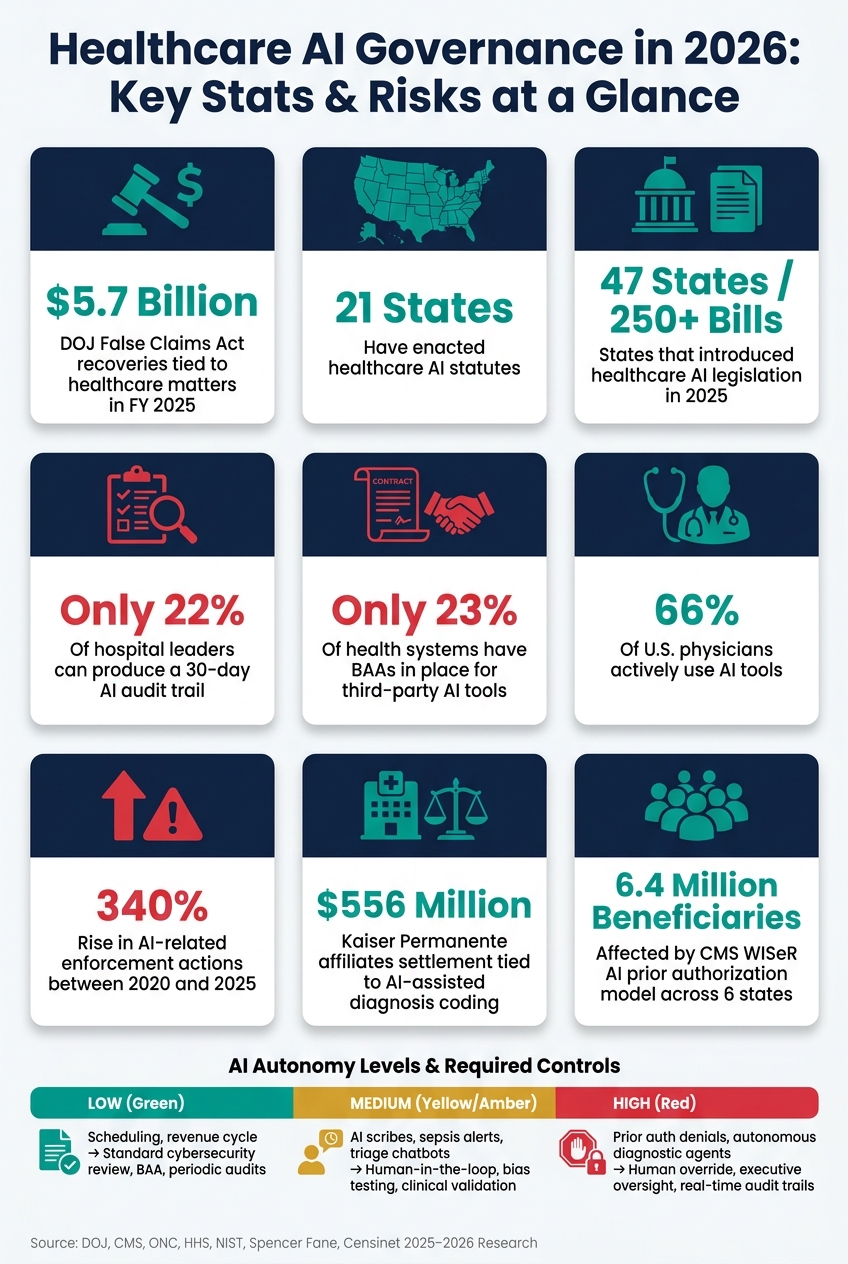
A few numbers show why this matters:
- $5.7 billion in DOJ False Claims Act recoveries tied to healthcare matters in FY 2025
- 21 states with healthcare AI statutes
- 47 states introduced 250+ healthcare AI bills in 2025
- Only 22% of hospital leaders said they could produce a 30-day AI audit trail
- Only 23% of health systems had BAAs in place for third-party AI tools, while 66% of U.S. physicians were using AI tools
Here’s the short takeaway: if I’m a healthcare leader in 2026, I can’t treat AI like a side project for IT. I need a formal review process, human accountability, vendor checks, drift monitoring, and records that show who approved what, who overrode what, and why.
| Pressure area | What changed in 2026 | What teams need to do |
|---|---|---|
| Federal oversight | Agencies expect documented review, clinician involvement, and traceable records | Build audit logs, review paths, and approval records |
| State laws | States now apply different AI rules to care, claims, and notices | Set one high bar across all markets |
| Clinical risk | AI errors, drift, and overreliance can affect patient care | Validate models and keep humans in charge |
| Privacy and cyber risk | Third-party and genAI tools can expose PHI and contract gaps | Review vendors, BAAs, and data use rules |
| Liability | Poor override and escalation rules create legal exposure | Assign owners and document decisions |
That’s the core message of the article: in 2026, healthcare AI governance becomes a day-to-day business, clinical, and compliance issue - not a future planning item.
Healthcare AI Governance in 2026: Key Stats & Risks at a Glance
What is pushing AI governance onto the 2026 agenda
Federal rules and guidance are setting concrete AI oversight expectations
By 2026, federal AI oversight in healthcare had moved from theory to day-to-day practice. The big shift is simple: agencies now expect proof. Not broad promises. Not loose internal policies. Actual oversight tied to care, payment, and records.
FDA guidance now limits opaque clinical decision support, and CMS rules require machine-readable prior authorization data, faster decisions, and a clinician - not AI alone - to make coverage calls [2][6]. That last point matters. An AI tool can support the process, but it can't be the final voice on coverage by itself.
AI-enabled medical products now also need Predetermined Change Control Plans (PCCPs). These are documented roadmaps that spell out how models may be updated without forcing a full new approval cycle every time [6]. In plain English, if a model changes, regulators want to know how, when, and within what guardrails.
ONC's HTI-1 rule, binding since January 2025, adds another layer. It enforces transparency and risk-management rules for predictive decision support tools built into certified health IT [1]. HHS Section 1557 nondiscrimination rules, applied as of May 2025, also reach AI-assisted clinical and administrative decisions [2].
Put together, these federal rules tie straight to clinical oversight:
- who reviews AI recommendations
- how coverage decisions get made
- what records must exist to show that process happened as required
State laws now add another layer of oversight that health systems and payers cannot standardize away.
State AI laws and payer rules are ending informal oversight
State action is making life harder for multi-state health systems in a very practical way. One state may focus on consumer notice. Another may focus on claims review. Another may target bias in insurer datasets. That means loose, informal AI oversight no longer holds up.
Colorado's SB 24-205 took effect on June 30, 2026, as the first broad U.S. statute aimed at "high-risk" AI. It requires healthcare deployers to complete formal impact assessments and provide consumer notifications when AI is used in consequential clinical or financial decisions [5]. Indiana's HB 1271, effective July 1, 2026, bars AI from serving as the sole basis for downcoding claims without professional review [4]. Alabama's SB 63, enacted in April 2026, requires health insurers to certify each year that their AI use does not rely on discriminatory group datasets and accounts for each beneficiary's unique clinical circumstances [4].
At the same time, CMS's WISeR model now uses AI in prior authorization across six states - New Jersey, Ohio, Oklahoma, Texas, Arizona, and Washington. It affects 6.4 million beneficiaries and pushes providers to recalibrate documentation so it can satisfy algorithmic reviewers [5].
That creates a messy operating picture. A health system can't just say, "We have one AI policy." It has to show that the policy works across different legal rules, payer demands, and review workflows.
Industry standards are raising the bar beyond minimum compliance
Laws and agency rules are only part of the story. Industry groups and professional bodies are also pushing expectations higher than bare-minimum compliance.
NIST-aligned AI risk management frameworks are being cited more often in state legislation, which turns what used to feel like optional best practice into something much closer to an enforceable duty for "high-risk" systems [5][3]. In healthcare, the push is heading in a clear direction: governance committees with cross-functional authority, documented validation, ongoing performance monitoring, and plain human oversight rules.
The gap between those expectations and actual readiness is still wide. Only 22% of hospital leaders said they could produce a 30-day AI audit trail [7]. That's the weak spot. Standards may ask for logs, review paths, and proof of oversight, but many organizations still can't pull that together on demand.
"AI in health care is not just a technology story; it is a governance story." - Christine Chasse, Attorney, Spencer Fane [2]
Those overlapping obligations create the clinical, privacy, and vendor risks discussed next.
sbb-itb-535baee
The main AI governance risks healthcare organizations cannot ignore
Clinical and generative AI create patient safety, privacy, and security gaps
These governance gaps tend to land in three places: patient safety, privacy, and liability.
At the point of care, clinical AI can fail when clinicians put too much trust in its recommendations. There’s also model drift, which can wear down accuracy over time. A tool that worked well at launch may not perform the same way months later.
Generative AI adds another layer of risk. If staff paste patient details into a large language model prompt to draft a clinical summary, that information may leak into training sets or reappear in inaccurate summaries. That’s not a small issue. It puts protected health information and clinical decision-making on shaky ground. The 2026 HIPAA Security Rule overhaul removes "addressable" safeguards and explicitly covers AI training data and prediction models [8].
The problem gets tougher when the AI is bought from outside vendors.
Third-party AI vendors expand cyber, privacy, and compliance exposure
Only 23% of health systems have Business Associate Agreements in place for their third-party AI solutions, even though 66% of U.S. physicians actively use AI tools [8]. That mismatch is a compliance problem sitting out in the open.
Most vendor security reviews were never built for AI. They often don’t ask basic but hard questions, such as:
- How was the model trained?
- Does it use patient data from other clients?
- What happens if the vendor ships a model update in the middle of the contract?
Then there’s the shadow-use problem. Clinicians or departments may start using AI tools without IT review or without a BAA. That opens the door even more. A health system can have a solid vendor review process on paper and still end up with unvetted AI running in parts of the enterprise. The covered entity still owns the risk.
AI liability grows when accountability and override rules are unclear
Liability grows fast when no one can show who reviewed AI outputs, who had the power to override them, or when escalation should have happened. If AI plays a part in a patient-safety event or a payment error, regulators and plaintiffs usually start with a blunt question: who was responsible for reviewing that output?
If there’s no clear human accountability, no override rules, and no escalation path, assigning liability gets messy fast.
The recent cases make that plain. In June 2026, Pennsylvania filed a lawsuit against Character.AI after the company's chatbots allegedly posed as licensed physicians, providing fake medical license numbers and clinical advice to users [2]. In early 2026, affiliates of Kaiser Permanente agreed to pay $556 million to resolve allegations involving unsupported diagnosis coding tied to Medicare Advantage reimbursement [2]. Both cases show how fast AI risk can snowball when human accountability rules, override requirements, and escalation paths are missing.
AI in Healthcare 2026: Governance, Clinical Safety & AI Agents Explained
What an effective 2026 AI governance program should include
Healthcare organizations need a formal operating model for AI. Ad hoc review won't cut it.
A cross-functional AI governance committee with clear authority
A formal governance committee closes that gap. And no, this can't be an IT-only steering group.
An effective committee brings together legal, compliance, IT, privacy, clinical leadership, and operations. Each group needs clear decision rights across the AI lifecycle. The committee should oversee intake, risk classification, ongoing monitoring, and documentation for every AI use case.
Accountability for AI-driven decisions stays with licensed clinicians [6][9]. AI cannot be the sole basis for coverage denials or medical necessity determinations [6][9]. The committee's role is to make sure that rule is baked into every deployment.
Once ownership is clear, the next move is turning that into policy.
Core policies, risk criteria, and controls for healthcare AI
A governance committee without written policies is just a meeting. The deliverables that matter most in 2026 are:
- Organizational AI policy
- Generative AI policy
- AI vendor due diligence standard
- Responsible data-use policy and model change controls
Risk classification is what drives the rest. Every AI tool should be reviewed against the same set of questions. Does it use PHI? What is its clinical impact? How much autonomy does it have? Is there bias risk? Does the vendor meet security and privacy requirements?
The table below links autonomy level to the controls each use case needs:
| AI Autonomy Level | Typical Use Cases | Required Controls |
|---|---|---|
| Low | Scheduling, revenue cycle, workflow automation | Standard cybersecurity review, vendor BAA, periodic performance audits [6][3] |
| Medium | AI scribes, sepsis alerts, triage chatbots | Documented human-in-the-loop, bias testing, patient disclosure, clinical validation [6][2] |
| High | Prior auth denials, autonomous diagnostic agents | Human override, executive oversight, audit trails, real-time transparency [6][3][9] |
State AI bills are still spreading. So if an organization sets its baseline to the toughest requirements now, it won't need to rebuild controls every time a new state law kicks in.
Monitoring, training, and incident response after deployment
Approval is only the first checkpoint. Monitoring starts at deployment.
Governance has to continue after go-live. A 2025 study across seven hospitals found a 0.12 AUROC drop after a routine lab-test change [7]. That's the kind of issue a one-time vendor review can miss. Continuous monitoring is what catches drift before it turns into a patient care problem.
Ongoing validation should include regular model performance reviews, periodic reassessment against updated clinical evidence, and logging that can reconstruct AI-driven decisions on demand. Only 22% of hospital leaders surveyed in late 2025 were highly confident they could produce a 30-day AI audit trail for regulators or payers [7].
Staff training matters just as much as policy. Clinicians need to know how to spot unreliable outputs and when to question the system. If something looks off, they should feel ready to act instead of assuming the tool must be right.
AI incident response plans need to exist before deployment. That includes defined escalation paths for unsafe outputs, clear workflows for privacy events tied to AI tools, and documented protocols for model drift or other post-deployment issues.
Put AI monitoring inside clinical quality dashboards and morbidity and mortality reviews.
That keeps AI governance inside daily clinical oversight instead of parking it off in IT.
How healthcare organizations can put AI governance into practice at scale in 2026
Once policy and oversight are in place, the next job is execution.
In 2026, healthcare teams need to turn governance into repeatable, auditable workflows across every AI use case. Put simply, governance can't live in a PDF or a committee charter. It has to show up in day-to-day work. That means centralizing intake, review, and remediation so the process holds up at scale.
Using Censinet RiskOps to centralize AI risk, policies, and remediation
A lot of governance programs look solid on paper and then fall apart in practice. Why? Because the work is scattered.
AI inventory sits in different places. Reviews drag on. Audit trails are thin. Remediation happens in fragments. Those gaps can weaken even a well-written program.
Use Censinet RiskOps as the system of record for AI assessments, exceptions, and remediation. The platform gives healthcare organizations one place to coordinate AI governance work. It routes critical findings to the right stakeholders, including AI governance committee members, for review and approval. And with real-time data in an AI risk dashboard, leadership can spot a high-risk vendor or an unresolved control gap right away.
Applying Censinet AI and Censinet AITM to speed third-party AI reviews with human oversight

Manual review hasn't kept pace with vendor volume.
Censinet AITM helps speed vendor review by summarizing evidence, recording integration details, and flagging third-party security threats, while still keeping human approval in the loop. Censinet AI supports human-reviewed automation for evidence validation, policy drafting, routing, and mitigation planning.
The difference in day-to-day operations is pretty clear:
| Governance Task | Manual Workflow | Human-Reviewed Automation (Censinet) |
|---|---|---|
| AI Inventory | Spreadsheets; prone to shadow AI gaps | Centralized RiskOps; captures clinical risk and ownership |
| Vendor Reviews | Months of back-and-forth emails | Censinet AITM summarizes evidence with human validation |
| Policy Drafting | Manual legal and compliance research | Censinet AI drafts policies based on specific risk criteria |
| Audit Readiness | Scrambling to collect point-in-time data | Continuous system of record with documented human overrides |
Christine Chasse of Spencer Fane notes that automated and semi-automated processes create major liability when organizations cannot show clinical support, traceability, and meaningful review [2].
Conclusion: The 2026 AI governance roadmap healthcare leaders should act on now
2026 is a convergence point.
Regulatory pressure, cybersecurity exposure, patient safety risk, and operational scale are all hitting at once. AI-related enforcement actions rose 340% between 2020 and 2025 [8], and the regulatory environment is getting more structured from here.
The organizations that come out ahead won't be the ones that adopted the most AI tools. They'll be the ones that built the governance infrastructure to manage those tools responsibly.
The path forward is concrete:
- Inventory every AI use case, including shadow AI
- Assign clear oversight authority
- Standardize third-party vendor risk management
- Monitor continuously after deployment
- Document every human override
The framework and tools are already here. What matters now is leadership urgency.
FAQs
What counts as AI in healthcare governance?
In healthcare governance, AI means a lot more than generative chatbots. It includes any machine-based system that looks at data and then produces predictions, recommendations, or decisions that shape clinical or operational workflows.
That covers both standalone tools and AI functions built into EHRs, imaging software, billing platforms, and admin automation. Governance also needs to account for risk level, plus new features that may show up through routine vendor updates.
How should we prioritize high-risk AI tools first?
Start with an enterprise-wide inventory of all AI already in use, including AI features tucked inside current platforms. Then sort each tool by how much it can affect patient care, reimbursement, and clinical outcomes.
Treat tools used for diagnosis, treatment, prior authorization, and patient-facing recommendations as high-risk. These tools need tighter controls. That means formal impact assessments, documented human oversight, and monitoring for clinical accuracy, bias, and performance drift.
What evidence should we keep for an AI audit?
Keep an audit-ready technical and operational record for each AI system. That record should cover the full picture, from how the model was built to how people supervise it day to day.
Include:
- The model’s purpose, data sources, training and validation characteristics, bias testing, and subgroup performance
- Human oversight records, such as operator competencies, override capabilities, and intervention logs
- Lifecycle monitoring, including performance, drift, incidents, system changes, and vendor agreements
This kind of record makes it much easier to trace what the system is supposed to do, how it has been checked, who can step in, and what has changed over time.
Related Blog Posts
- AI Governance Talent Gap: How Companies Are Building Specialized Teams for 2025 Compliance
- AI Vendor Risk Management in Healthcare: The Complete 2025 Governance Guide
- The AI Governance Revolution: Moving Beyond Compliance to True Risk Control
- The Regulated Future: How AI Governance Will Shape Business Strategy
