Medical device access control is critical for protecting patient safety, healthcare operations, and sensitive data. Weak access controls can lead to data breaches, device tampering, and even patient harm. This guide covers essential practices, regulatory requirements, and actionable steps for securing medical devices throughout their lifecycle.
Key Takeaways:
- Why It Matters: Poor access controls can lead to patient harm, data breaches, and operational disruptions.
- Shared Responsibility: Security involves both manufacturers (design, updates) and healthcare organizations (implementation, management).
- Regulations: Compliance with FDA, HIPAA, and global standards like IMDRF ensures devices are secure and meet legal requirements.
- Best Practices: Role-based access, strong authentication, network segmentation, and continuous monitoring are essential.
- Lifecycle Approach: Security starts at procurement and continues through onboarding, daily use, and decommissioning.
Access control isn't a one-time task - it requires continuous effort and collaboration. Below, you'll find practical insights and steps to safeguard medical devices effectively.
Regulatory and Standards Foundations for Access Control
Key Frameworks for Access Control
Access control in medical devices is shaped by a mix of laws, guidance documents, and international standards. These frameworks require collaboration between manufacturers and healthcare organizations to ensure compliance.
In the U.S., Section 524B of the FD&C Act, introduced through the 2023 Omnibus spending bill, plays a central role. It mandates that sponsors of "cyber devices" include cybersecurity details, such as access control plans and a software bill of materials (SBOM), in their premarket submissions like 510(k), PMA, and De Novo applications [1]. According to the FDA:
"The sponsor of a premarket submission for a cyber device must include information to demonstrate that the cyber device meets the cybersecurity requirements in section 524B(b) of the FD&C Act." [1]
Since October 1, 2023, the FDA has implemented a "Refuse to Accept" policy for submissions that fail to meet these requirements. Guidance finalized on June 27, 2025, outlines expectations for device design and labeling to align with these rules [1][5].
On a global scale, the International Medical Device Regulators Forum (IMDRF) provides complementary guidance. Key documents include N60, which lays out general cybersecurity principles; N70, which addresses security challenges for legacy devices; and N73, which focuses on SBOM best practices [2][6][7]. Together, these frameworks emphasize the importance of integrating strong access controls throughout a device's lifecycle.
How HIPAA and CMS Requirements Apply
Access control isn't just about premarket submissions - it’s also critical for data protection. While the FDA oversees device design and premarket compliance, HIPAA's Security Rule governs how healthcare organizations protect the data these devices handle. For devices managing protected health information (PHI), HIPAA requires access to be controlled, monitored, and auditable. Similarly, CMS regulations hold healthcare providers accountable for implementing effective access control measures.
The 2023 amendments to the FD&C Act expanded the FDA's authority to address non-safety security risks, including PHI protection. This aligns device security requirements more closely with HIPAA's objectives [3]. Device labeling also plays a critical role here. If a device's labeling fails to provide clear instructions for authentication settings or configuring access controls, it could be deemed "misbranded" under the FD&C Act [3][4]. Manufacturers must ensure that their documentation is detailed enough to allow healthcare IT teams to manage these settings effectively, bridging FDA and HIPAA compliance requirements.
Mapping Standards to Device Security Requirements
U.S. laws and global standards converge to define access control requirements clearly. The table below highlights key frameworks and their focus areas:
| Framework / Standard | Focus Area | Access Control Requirement |
|---|---|---|
| FD&C Act Section 524B | Statutory law | Requires cybersecurity plans and SBOMs in premarket submissions [1] |
| FDA Guidance (June 2025) | Regulatory expectations | Device design, labeling, and quality system documentation [5] |
| HIPAA Security Rule | PHI protection | Controls to prevent unauthorized access to health data on devices [3] |
| IMDRF N60 | Global principles | General cybersecurity practices across the device lifecycle [2] |
| IMDRF N70 | Legacy devices | Managing access control on older, unsupported medical equipment [6] |
| IMDRF N73 | SBOM | Tracking software components to identify and manage access-related vulnerabilities [7] |
| AAMI TIR57 | Security risk management | Separate security risk process, distinct from safety risk (ISO 14971) [3] |
AAMI TIR57 emphasizes the importance of separating security risk management from safety risk management under ISO 14971 [3]. This distinction is vital for access control because security failures - like unauthorized remote access - might not trigger safety alarms but can still result in significant harm. By addressing critical medical device security risks independently, organizations can better safeguard both device functionality and patient data.
sbb-itb-535baee
Technical Best Practices for Medical Device Access Control
Role-Based and Least-Privilege Access
Effective access control begins with clearly defined user roles, ensuring device functionality and patient safety are protected. This involves mapping permissions to specific roles - like clinicians, biomedical engineers, IT staff, and third-party vendors - so each group only has access to the resources they need. Christian Espinosa, Founder & CEO of Blue Goat Cyber, highlights the importance of this approach:
"Least privilege can be one of the last defenses for a cyber-attack. If there's a credential breach, the threat actor may realize they have minimal access and cannot infiltrate the medical device's software or network." [10]
To strengthen role-based access control (RBAC), organizations should adopt two important practices. First, implement just-in-time (JIT) privilege elevation to provide temporary administrative access only when necessary, automatically revoking it after a set period [8]. Second, enforce segregation of duties by dividing responsibilities among clinical engineering, IT security, and vendor teams, reducing the chances of any single account becoming a weak point [8]. Emergency access should follow strict "break-glass" protocols, requiring multi-factor authentication, short access durations, and mandatory audits of all activity [8].
These measures create a strong foundation for managing credentials and securing networks, which are detailed in the next sections.
Strong Authentication and Credential Management
Default credentials set by manufacturers are a well-known security risk. To mitigate this, replace default credentials with unique, per-user accounts and use automated credential rotation instead of shared or static passwords [8]. For maintenance tasks, static master PINs should be swapped out for one-time or short-lived codes tied to the specific user, device, and task [8]. Sensitive actions should incorporate identity providers to enforce robust authentication protocols [8].
For portable or mobile medical devices, Mobile Device Management (MDM) or Unified Endpoint Management (UEM) platforms can enforce password complexity, limit access to applications, and enable remote data wiping if a device is lost or compromised [9]. Additionally, setting up automatic inactivity timeouts ensures unattended devices don't become an entry point for unauthorized access [10].
While strong authentication is essential, securing the network environment is equally critical, as described below.
Network-Level Access Control and Monitoring
Even the strongest authentication measures can be undermined by a vulnerable network. Hospitals typically manage 10 to 15 connected medical devices per patient bed, creating a large attack surface that must be carefully managed [9]. Network segmentation, achieved through VLANs and firewalls, helps contain malware by preventing lateral movement. Zero Trust principles further secure the environment by treating every connection as untrusted until verified. A centralized SIEM system adds another layer of protection by continuously analyzing logs and issuing real-time alerts [9].
This layered approach is particularly important for legacy devices that lack modern authentication capabilities. By isolating these devices through segmentation, organizations can minimize risks even when updates or patches are unavailable [9]. The March 2026 Stryker cyberattack, which caused a global system outage and led to the remote wiping of tens of thousands of employee devices, serves as a stark reminder of the importance of internal network controls alongside vendor-side measures [9].
Regular use of automated network discovery tools is also essential to maintain a complete and accurate inventory of all connected Internet of Medical Things (IoMT) devices [11].
| Measure | Implementation | Primary Benefit |
|---|---|---|
| Network Segmentation | VLANs and firewalls | Prevents lateral movement of ransomware |
| MDM/UEM | Centralized policy enforcement | Ensures devices only connect to approved networks |
| Zero Trust | Identity-based, continuous verification | Restricts access to only what is necessary |
| SIEM Monitoring | Log aggregation and real-time alerts | Provides early warning of unauthorized access |
| Automated Discovery | Regular IoMT network scans | Maintains an accurate inventory for visibility |
To tie these technical practices into a larger security framework, healthcare organizations can rely on risk management platforms like Censinet RiskOps™. These platforms streamline third-party and enterprise risk assessments while offering continuous oversight of medical device ecosystems.
Security Architecture Views: Protecting Medical Devices Through Strategic Design
Integrating Access Control Across the Medical Device Lifecycle
Medical Device Access Control: Lifecycle Security Best Practices
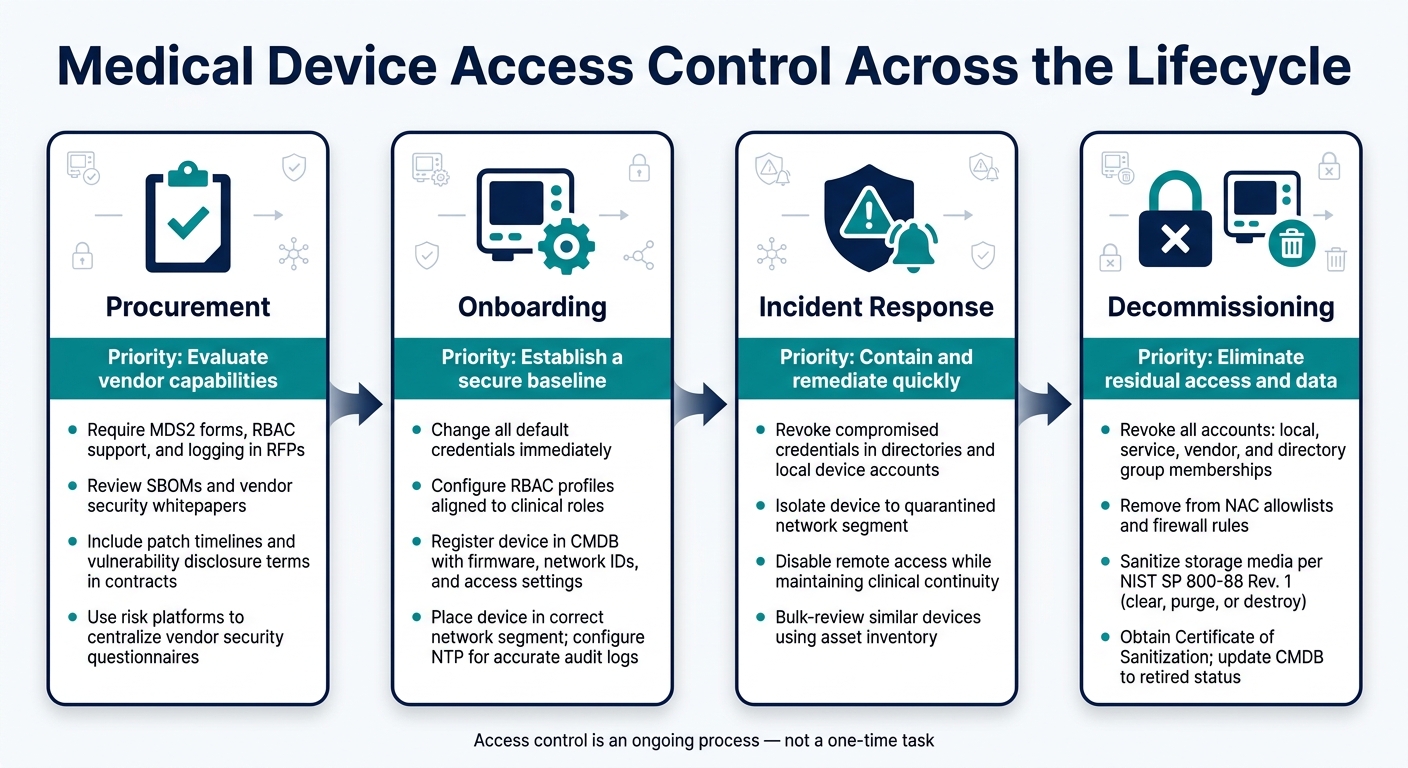
Access control isn't something you can configure once and forget - it needs to be actively managed throughout a device's entire lifecycle, from the moment it's procured to when it's finally decommissioned. Organizations that treat access control as an ongoing process are better equipped to manage risks and avoid reacting to security incidents after they've already occurred. By taking this lifecycle approach, you can connect early vendor assessments with long-term operational security. Here's how it all comes together.
Procurement and Vendor Evaluation
The journey starts at procurement. This is when you set the stage for strong access control by defining clear security requirements. Procurement documents should demand that vendors support features like unique user IDs, configurable role-based access control (RBAC), strong authentication, centralized logging, and directory integration. Contracts and Business Associate Agreements (BAAs) should also include specific timelines for patches, requirements for vulnerability disclosures, and expectations for log retention.
The Manufacturer Disclosure Statement for Medical Device Security (MDS2) is an excellent tool for procurement teams. It provides a standardized way to evaluate whether a device supports key security features like authentication, audit controls, and authorization. Reviewing MDS2 forms alongside Software Bills of Materials (SBOMs) and vendor security whitepapers can help you identify gaps in access control before making any purchase decisions. Tools like Censinet RiskOps™ simplify this process by centralizing security questionnaires and evidence collection.
Secure Onboarding and Device Configuration
Once a device arrives, it needs to go through a standardized onboarding process to ensure it’s secure from the start. This includes changing default credentials and configuring RBAC profiles that align with actual clinical roles, such as nurses, respiratory therapists, biomedical engineers, or vendor technicians. Each role should only have the minimum privileges necessary to perform its tasks.
At this stage, you should also register the device in the Configuration Management Database (CMDB). Record key details like the owning department, device type, firmware version, network identifiers, supported authentication methods, and current access control settings. This information becomes critical for audits, incident response, and managing changes over time. Devices should also be placed in the correct network segment and registered with Network Access Control (NAC) systems. Don’t forget to configure Network Time Protocol (NTP) to ensure that all audit logs have accurate timestamps.
By setting up secure onboarding processes, you’re laying the foundation for effective incident response and smooth decommissioning if vulnerabilities are discovered later.
Incident Response and Device Decommissioning
If there’s a suspected credential compromise or evidence of device tampering, swift action is essential. Start by revoking compromised credentials in both centralized directories and device-local accounts. Isolate the device by moving it to a quarantined network segment, and disable remote access channels while ensuring clinical operations can continue. Using the asset inventory, you can quickly identify other devices of the same model that might share accounts or vulnerabilities, allowing for bulk access reviews tied directly to device records.
When it’s time to decommission a device, every logical access point must be revoked - this includes local accounts, service accounts, vendor credentials, and directory group memberships. Remove the device from NAC allowlists and firewall rules. For storage media, follow the NIST SP 800-88 Rev. 1 guidelines to sanitize data. Depending on the sensitivity of the data, you might choose to clear, purge, or destroy the media. If you’re using a third-party disposal vendor, make sure to get a formal Certificate of Sanitization that includes the device’s serial number and the erasure method used. Finally, update the CMDB to reflect the device’s retired status, completing its lifecycle record.
By maintaining access control throughout the device's lifecycle, you reduce risks at every stage - from procurement to decommissioning.
| Lifecycle Stage | Access Control Priority | Key Action |
|---|---|---|
| Procurement | Evaluate vendor capabilities | Require MDS2, RBAC, logging, and directory integration in RFPs |
| Onboarding | Establish a secure baseline | Change defaults, configure RBAC, register in CMDB, enable log forwarding |
| Incident Response | Contain and remediate quickly | Revoke credentials, isolate device, review logs, check similar devices |
| Decommissioning | Eliminate residual access and data | Revoke all accounts, sanitize media per NIST SP 800-88, update inventory |
Building a Culture of Secure Access Control
Relying solely on technical controls won't cut it if users don't understand their role in maintaining access security. Creating a culture of secure access means embedding security practices into everyone's daily habits - not just leaving it to the IT department.
Training and Awareness Programs
Effective training tailored to specific roles is critical for all staff - whether they're clinicians, IT professionals, or biomedical engineers. This ensures everyone understands their responsibilities when it comes to secure access. Training should align with the Shared Responsibility Model introduced earlier. When teams clearly know which access control tasks fall to them, the device manufacturer, or IT, it minimizes confusion and plugs gaps that attackers often exploit.
Short, scenario-based sessions work better than annual compliance reviews, especially in fast-paced clinical settings where time is limited. These shorter, targeted trainings are more practical and impactful.
To ensure progress, it's important to track performance using specific metrics tied to access control.
Metrics and KPIs to Track
The right metrics can show whether your access control program is genuinely effective or just looks good on paper. Here are some key indicators to monitor:
- MFA enrollment rate for devices in scope
- Time to revoke access for users who leave the organization (commonly referred to as the "leaver workflow")
- Percentage of accounts mapped to RBAC roles, tracked quarterly, along with dormant account rates
- Frequency of "break-glass" access events and whether each instance undergoes a review
One of the best ways to improve the time-to-revoke metric is by automating joiner-mover-leaver workflows using HR data. Studies in large healthcare organizations reveal that manually managing access policy changes can take up to 6.67 support hours daily [12]. Automation significantly reduces this time and effort.
To manage these metrics effectively, healthcare organizations should leverage tools that provide automated and continuous monitoring.
Using Risk Intelligence Platforms
Manually tracking metrics across a large fleet of devices is neither efficient nor practical. Risk intelligence platforms, like Censinet RiskOps™, simplify this process by offering a centralized view of access control across IT and clinical environments. These platforms help bridge the gap between IT and biomedical engineering teams, breaking down traditional silos.
Instead of relying on occasional audits, these platforms enable continuous monitoring. They allow organizations to track how access control risks evolve as new devices are introduced or firmware updates are applied. Additionally, during procurement, these tools automate the collection of vendor security documentation. This ensures that access control requirements are met before a device is even deployed. Risk scores generated by the platform can also guide purchasing decisions, favoring devices with features like enterprise SSO, MFA, and modern RBAC capabilities.
"Identity decisions that ignore context create either friction or exposure." - NHI Mgmt Group Editorial Team [13]
This balancing act is especially challenging in healthcare. The aim isn't to make access so restrictive that clinicians find ways to bypass it. Instead, the goal is to make secure access the easiest, most convenient path - supported by visibility and data to confirm it's working. By blending cultural practices with technical solutions, organizations can maintain strong access control throughout the lifecycle of medical devices.
Conclusion
Managing access control for medical devices is not a one-and-done task - it’s an ongoing process that spans the entire lifecycle of the device. The risks are high: unauthorized changes to a device’s settings can directly impact patient safety. Imagine an infusion pump’s dosing limit being tampered with or a ventilator’s parameters being altered without proper authorization. These are not hypothetical scenarios - they’re real threats.
The regulatory landscape is evolving to address these risks. Starting February 2, 2026, the FDA’s updated Compliance Program Manual (#7382.850) will require manufacturers to integrate cybersecurity measures into their quality management systems throughout a device’s lifecycle [4]. Naomi Schwartz, VP of Regulatory Strategy at Medcrypt, emphasizes this shift perfectly:
"The cost of compliance outweighs the cost of a breach, which risks brand reputation at best and patients' lives at worst." [14]
To build a solid foundation for access control, organizations should focus on key practices like least-privilege access, unique user credentials paired with Multi-Factor Authentication (MFA), automated de-provisioning, and maintaining a real-time inventory of devices. These strategies align with a Zero Trust framework, which minimizes an attacker’s ability to move laterally within a compromised system.
Platforms such as Censinet RiskOps™ are designed to help healthcare organizations implement these principles effectively. They offer centralized tools to monitor vendor security postures, automate risk assessments, and ensure continuous oversight of access control settings. From the initial evaluation of a device to its eventual decommissioning, this lifecycle-wide approach enables proactive risk management - setting apart organizations that stay ahead of threats from those that merely respond to them.
FAQs
What medical devices are considered “cyber devices” under FDA Section 524B?
According to FDA Section 524B, a cyber device is defined as any medical device that meets these three criteria:
- It includes sponsor-validated software as part of or within the device.
- It connects to the internet.
- It has technological features, approved by the sponsor, that could be exposed to cybersecurity threats.
This definition also applies to devices that use wireless protocols like Bluetooth or physical connectors such as USB.
How can hospitals use RBAC and MFA without slowing down clinical care?
Hospitals can streamline clinical workflows while maintaining security by implementing access policies that adjust based on risk. For shared workspaces, combining badge tap-and-go technology with PINs or biometrics allows for fast and secure authentication. To protect highly sensitive actions, such as exporting Protected Health Information (PHI) or accessing systems on unmanaged devices, step-up multi-factor authentication (MFA) can be deployed selectively.
To further enhance efficiency, enabling session roaming ensures clinicians can switch devices seamlessly without losing progress. Additionally, using short re-authentication grace periods minimizes workflow interruptions while keeping security standards intact. This balance of convenience and protection helps healthcare professionals stay focused on patient care.
What should we do when a device can’t support modern authentication?
If a medical device lacks support for modern authentication, consider implementing Zero Trust Architecture. This method ensures secure connections by continuously verifying identity, device health, and compliance with security policies at the infrastructure level. To achieve this, tools like Public Key Infrastructure (PKI) and digital certificates can automate authentication processes effectively.
To further enhance security, apply network micro-segmentation. This technique isolates older or high-risk devices, minimizing the chances of breaches and containing any potential threats within specific areas of the clinical network.
