AI is already in many U.S. hospitals, but board-level control is still thin. By 2024, 71% of hospitals were using predictive AI in the EHR, yet only 18% of health system executives said their AI governance was mature, and nearly 50% of boards and executive teams were not discussing AI at all.
If I had to sum up the article in one line, it would be this: healthcare leaders need a repeatable AI oversight program, not a one-time AI lesson. The article lays out a seven-part webinar series built to help hospitals move from scattered AI use to one review path that covers:
- governance and ownership
- risk assessment using NIST AI RMF
- HIPAA, PHI, and data-use review
- third-party and vendor risk checks
- incident response
- board dashboards and reporting
- workflow support through Censinet tools
The main point is simple: if you don’t know what AI tools are in use, who approves them, what data they touch, how vendors change them, and what happens when they fail, you don’t have AI oversight yet.
A few facts make that gap hard to ignore:
- Billing automation use rose from 36% to 61%
- Scheduling AI use went from 51% to 67%
- 51% of healthcare groups still rely on ad hoc discovery to find AI tools
- More than 90% lack automated AI product monitoring
What I like about the piece is that it stays focused on action. Instead of repeating AI buzzwords, it points leaders toward plain next steps: build an inventory, set owners, tier risk, review PHI use, tighten vendor terms, log incidents, and report clear metrics to the board.
In short, this is less about “learning AI” and more about running AI like any other high-risk hospital function.
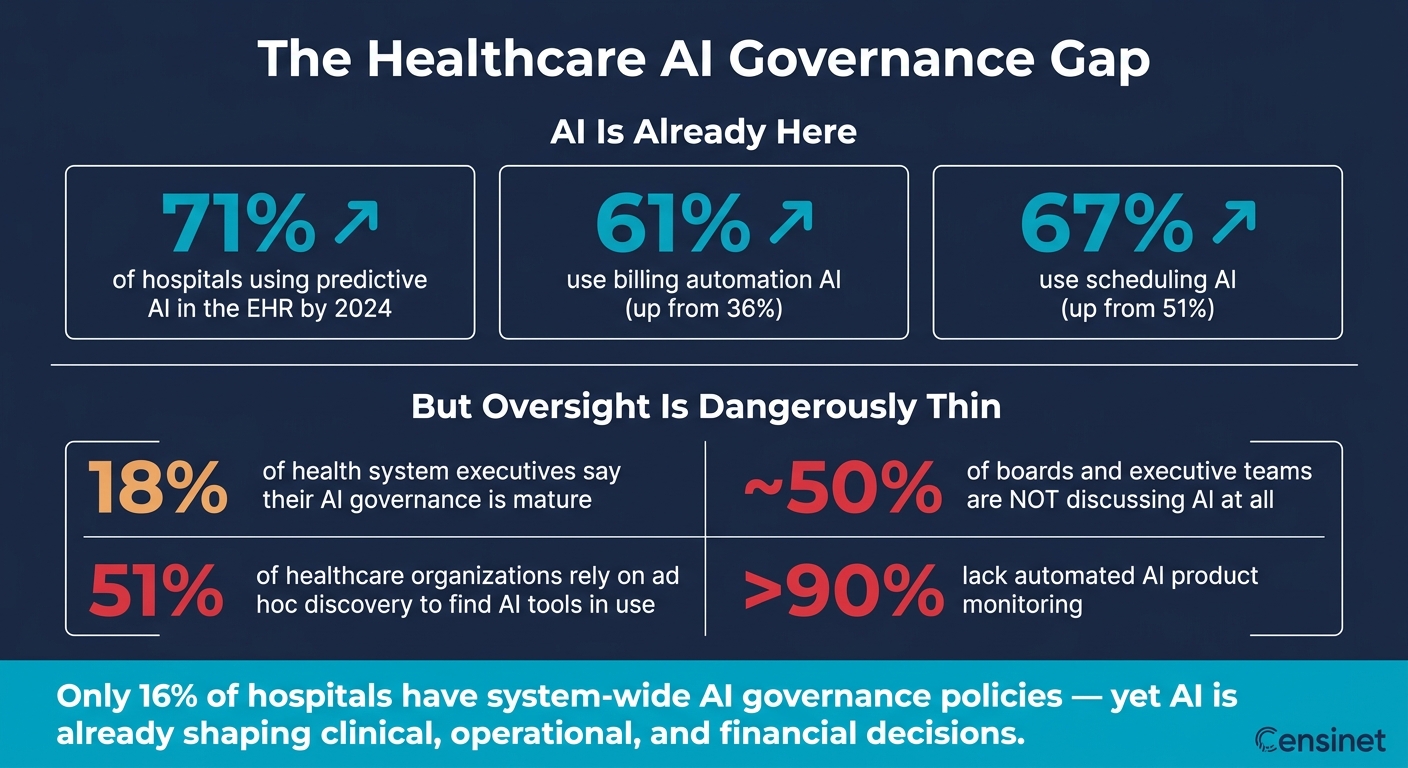
Healthcare AI Governance Gap: Key Statistics at a Glance
Healthcare AI Governance - Risks, Compliance, and Frameworks Explained
sbb-itb-535baee
Why a Webinar Series Works Better Than One-Off AI Training
A single training session can build awareness. But AI governance in hospitals and health systems calls for a process that covers risk, privacy, vendor review, cybersecurity, incident response, and board reporting.
Those areas don’t sit in separate boxes. The way you build a model inventory affects how you run risk assessments. The way you handle privacy review shapes what you can approve during procurement. Pull one thread, and the others move with it.
That’s why a structured series works better. It matches how governance happens in practice: start by building shared language, then move into tool review, vendor review, and control decisions. Skip that groundwork, and teams often approve tools ad hoc. The result is messy: inconsistent controls, blurry accountability, and unsanctioned AI use across departments.
Each session should lead to one usable deliverable, such as:
- a charter
- a template
- a questionnaire
- a playbook
- a draft board dashboard
That way, every session gives the group something concrete to use in the next one.
The NIST AI RMF is built to work across the AI lifecycle, not as a set of isolated steps. That gives leaders one way to think across clinical, operational, and vendor reviews. CHAI’s governance framework takes a similar path, with a focus on continuous monitoring, risk-based management, and multidisciplinary oversight. A webinar series gives clinical, compliance, IT, legal, and security teams time to absorb each concept and put it into practice before moving on.
There’s also a simple reason this format fits healthcare. Like HIPAA refresher training, AI governance needs repeated review because models, new vendors, and regulations keep changing. Recurring sessions help keep policies lined up with those changes. That’s why the series starts with a governance operating model before moving into risk, privacy, and vendor review.
1. Censinet Session: Building a Healthcare AI Governance Operating Model
Before a health system starts scaling AI, leadership needs straight answers to three basic questions: Who approves use? How are requests reviewed? What controls apply? If those answers aren't set upfront, teams make their own rules. That's when shadow AI use starts creeping in, and risk decisions get made unevenly across departments. A clear model turns AI review from an ad hoc approval process into a repeatable workflow.
A governance operating model gives those decisions a fixed place to live. Research on AI governance in a large health system found that a lack of clear accountability and fragmented oversight can slow AI deployment and increase risk.[5]
Once ownership is set, the next job is deciding what the model needs to control. It should cover six risk domains:
- patient safety
- clinical quality
- privacy and HIPAA compliance
- cybersecurity
- bias and fairness
- operational reliability
The risk profile changes with the use case. Ambient documentation brings accuracy and privacy concerns. Triage tools bring patient safety, bias, and escalation concerns. Revenue-cycle automation may seem less clinical, but it can still lead to denials or scheduling errors.
Ownership also needs to be mapped across clinical, IT, security, compliance, legal, procurement, and the business side. Clinical leaders review patient-safety impact. IT and security look at technical controls. Compliance and legal handle HIPAA and regulatory exposure. Procurement manages contract protections. Named business owners stay on the hook for performance after deployment. The ONC HTI-1 Final Rule lines up with this approach by adding DSI requirements for predictive AI in certified EHR technology, including risk analysis, mitigation, and governance controls.[1][2][3]
The outputs from this session become the base for later risk, privacy, and vendor sessions. That includes an AI use-case inventory, a risk-tiering template, a one-page intake form that shows whether a system touches PHI or affects patient care, an approval checklist, and an exception log. Censinet RiskOps™ supports this work as a central hub for AI-related policies, risks, and tasks. It routes issues to the right owners, so accountability stays clear as the series moves into risk assessment, privacy review, and vendor oversight.
2. How to Run AI Risk Assessments Using NIST AI RMF and Healthcare Standards
Once your governance model is in place, the next step is simple in theory and hard in practice: assess risk the same way across every AI system your organization uses or plans to use. That’s where the NIST AI Risk Management Framework (AI RMF) helps. It gives you a repeatable review structure, so AI oversight works like a hospital process, not a one-off exercise. Use the inventory from the governance session to score each system with the same lens.
The AI RMF breaks risk assessment into four functions: Govern, Map, Measure, and Manage.
Under Govern, leaders set the rules for AI acquisition, validation, monitoring, retirement, acceptable risk thresholds, and escalation paths for high-risk systems. Under Map, teams document what each AI system does, including its inputs, outputs, affected populations, business value, and data sources. Under Measure, they choose the metrics that matter, such as model bias rates, false-negative rates, uptime, explainability scores, and performance by demographic subgroup. Under Manage, they define remediation timelines, change management steps, and incident response actions for cases where a model fails or drifts.
A practical healthcare AI risk assessment should begin with an AI system inventory. Classify each tool by ePHI exposure, clinical impact, and vendor transparency. Then tier systems as low, medium, high, or critical based on severity, likelihood, reversibility, and data sensitivity. A patient-facing sepsis alert model belongs in a very different risk tier than an internal scheduling optimization tool. The level of review should match that gap.
The assessment should cover six healthcare-specific domains:
- Clinical safety and efficacy
- Data protection and HIPAA compliance
- Bias and health equity
- Cybersecurity and system integrity
- Operational resilience and workflow impact
- Legal, regulatory, and reputational risk
Each use case - whether it is an ED triage model, an automated prior authorization tool, or a patient chatbot - should be reviewed across all six domains before deployment. In plain terms, don’t just ask whether the model works. Ask whether it is safe, whether it handles data the right way, whether it performs evenly across groups, and what happens if it breaks at the worst possible moment.
You should also map the AI RMF to the healthcare rules and expectations that already shape your risk program. That includes HIPAA Security Rule safeguards, FDA expectations for diagnosis or treatment tools, Joint Commission safety and quality requirements, and HIPAA breach-response duties.
The outputs need to be concrete and reusable, not buried in slide decks. Teams should produce model cards that summarize training data, performance across subpopulations, intended use, and known limits. They should also create threat and hazard registers, approval logs with deployment conditions, and monitoring dashboard specs that spell out which metrics go to executives and how often. Keep all of these artifacts in one audit-ready record. Those records then feed the HIPAA and data-use review that comes next.
3. HIPAA, Data Use, and Privacy Oversight for AI
The risk assessment from the last section leads straight into a tougher issue: what data moves through your AI systems, and do you have the legal and day-to-day controls to govern it? Once a use case is scored for risk, privacy review decides whether it can move ahead. That risk tier now shapes how deep the privacy review needs to go. HIPAA still applies to any AI tool that accesses, processes, or generates outputs from protected health information (PHI), and AI does not create new exceptions to those rules [6][7].
Before approving any tool, map the data. Leaders need a clear view of whether the use case involves PHI, who the covered entity is, who the business associate is, and whether the tool creates new disclosures. That review should cover training data, prompts, outputs, logs, and retention. A vendor saying a product is HIPAA-ready is not the same as having contract terms that your team has actually reviewed.
Generative AI brings risks that fixed-rule software does not. Old-style software tends to behave within set instructions. A generative model can store prompts, return unexpected outputs, and expose PHI through vendor telemetry or model logs in ways staff may not expect. One problem stands out: prompt leakage. That happens when an employee pastes patient details into a public AI tool without realizing the data may be kept outside the organization. In healthcare, that is not a small slip. OCR enforcement makes it clear that HHS takes privacy and security failures seriously. So documentation is not busywork. It is a control.
Required proof of oversight includes:
- a data-flow map
- a privacy impact assessment
- a risk assessment
- a business associate agreement where needed
- documented sign-off from compliance, security, and operational owners
For higher-risk tools, leaders should also ask for records showing allowed data elements, retention limits, access controls, and the steps the organization will take if the tool misuses or exposes PHI.
Use the decision areas below to check whether governance is covered:
| Governance Decision | What Leaders Need to Verify |
|---|---|
| PHI in training or fine-tuning | Documented approval, de-identification validation, privacy review on file |
| Vendor-hosted AI with PHI access | BAA in place, subprocessor list reviewed, data retention and deletion terms confirmed |
| Staff use of generative AI tools | Approved use-case list, prohibition on public tools for PHI, monitoring for misuse |
| De-identification for AI datasets | Expert determination or safe harbor method documented - not just vendor assurance |
| Patient-facing AI outputs | Human review process, output sampling, consent or notice requirements addressed |
De-identification is a common blind spot. HIPAA's Expert Determination method requires a human expert to certify low re-identification risk and document the method [8][9]. Removing names alone is not enough. A dataset can still point back to a person when dates, rare diagnoses, and geographic data are combined. That is why leaders should require a formal privacy review before treating any AI training dataset as safe just because the obvious identifiers are gone.
Privacy oversight also breaks down when it lives only in IT. Compliance, legal, security, clinical leadership, and data owners all need a seat at the table. Just as important, they need a shared intake process that sends low-risk uses through a lighter review and routes PHI-heavy or patient-facing tools through a formal approval path. That keeps review moving for lower-risk work without going soft on tools that touch patient data. Once data use is clear, vendor access and subcontractor controls become the next layer to review.
4. Managing Third-Party and AI Vendor Risk Across the Supply Chain
Once data use gets approved, the next risk layer is vendor oversight. Most healthcare groups already have some kind of third-party risk review in place. But the usual vendor check often misses AI-specific issues.
A standard security questionnaire won't ask if a vendor retrains its model without telling you. It also may not ask whether the platform relies on an embedded third-party model that brings clinical risk no one reviewed. At that point, vendor oversight isn't just about the vendor. It's about who else can touch the data and how the model might change over time.
The stakes aren't abstract. Ponemon Institute research found that 36% of healthcare organizations and 55% of business associates link privacy and security incidents to third-party failures [13]. The Health Sector Coordinating Council's 109-page Third-Party AI Risk and Supply Chain Transparency Guide points to embedded models and subprocessors that create hidden risk, including possible clinical and cybersecurity harm [10][12]. NIST AI RMF guidance published through 2025 also moved supply chain and third-party model assessment into the top tier of concern [11]. Contracts should require notice of retraining, training-data changes, and new subprocessors.
Use these questions during procurement before approving any AI tool:
| Due Diligence Domain | AI-Specific Question for Vendors |
|---|---|
| Model Governance | Does the vendor notify you when models are retrained or updated? |
| Supply Chain | What open-source dependencies or third-party subprocessors are used in the AI stack? |
| Security | How does the tool protect against prompt injection and model poisoning? |
| Autonomous-agent risk | What elevated permissions do autonomous agents have, and how is agent hijacking prevented? |
| Compliance | Does the vendor support HIPAA terms, audit rights, and change notifications for model updates and subprocessors? |
| Lifecycle | What is the formal process for decommissioning the AI tool and purging associated data? |
IT can't handle this review by itself. Clinical, compliance, legal, procurement, and security teams need to share intake, approve AI-specific terms, and make risk calls through one governance group. That should include model-training limits, subprocessor disclosure, and data-use restrictions. The same group should also rely on the vendor record during incident response if the tool fails or changes without warning.
Censinet RiskOps™ can route findings to compliance, security, and clinical owners and keep third-party AI risk in one dashboard.
5. Incident Response and Resilience for AI-Enabled Systems
Vendor review helps catch risk before a tool goes live. But deployment is where things get real. When an AI system fails, the event might turn into a clinical issue, an ops outage, a cyber event, or a compliance problem. Each one follows a different path. That’s why AI incidents should move through the same security, breach, and patient safety workflows the organization already uses, not a separate AI track. In practice, incident response shows whether AI governance holds up once the tool is in use.
Set the rules before an incident happens. Decide who has the authority to deactivate an AI tool in production. NIST AI RMF calls for bypass and deactivation procedures, along with backup workflows for mission-critical AI.[14] Once that authority is clear, the next step is just as important: keeping enough evidence to piece together what happened.
AI logs should record model version, inputs, timestamps, confidence scores, and clinician overrides. Put that requirement directly into the vendor contract, BAA, and onboarding checklist.
Cross-functional drills help teams find weak spots early. A tabletop exercise where IT, the CISO, the CMO, compliance, and legal work through a realistic event - like a ransomware attack that knocks out an AI triage tool - can expose problems no policy document will spot.[15] A common issue is blurry clinical authority to stop an AI tool. Another is poor handoff between the incident command team and frontline clinicians. Both need to be nailed down in advance.
The table below maps the four core AI incident categories to the teams that lead them and the evidence that should be kept:
| AI Incident Type | Lead Response Team | Evidence to Capture |
|---|---|---|
| Clinical safety (e.g., suppressed alerts, incorrect recommendations) | CMO, Chief Quality Officer | Model version, inputs, confidence scores, clinician overrides, timestamps |
| Operational reliability (e.g., scheduling tool failure during peak hours) | CIO, Operations | Uptime logs, error reports, downstream impact data, fallback workflow records |
| Cybersecurity & integrity (e.g., model poisoning, vendor breach exposing PHI) | CISO, SOC | Access logs, anomaly alerts, vendor incident reports, chain-of-custody documentation |
| Privacy and compliance (e.g., PHI stored outside the approved data region) | CPO, HIPAA Privacy & Security Officer, Compliance Officer | Data flow records, authorization scope, breach risk assessment, notification timeline |
Those records also feed executive dashboards and board reporting.
6. Board-Ready Oversight and Executive Dashboards for Healthcare AI
Once incident records are in place, bring them together in one executive dashboard. That matters because a 2024 governance-focused survey found that only 16% of hospitals had system-wide AI governance policies in place, even while boards are being asked to oversee AI systems they rarely see up close.[17] The answer is a standard dashboard that gives leaders one clear view.
Keep the layout consistent, and add short narrative notes under each category. For board review, organize AI risk in this order: patient safety and clinical quality, data privacy and HIPAA compliance, cybersecurity and resilience, third-party and vendor exposure, and regulatory and legal risk. Use red/yellow/green status flags so directors can scan the page fast. Then add one short action note for each metric. That way, the dashboard doesn't just show problems. It shows what happens next.
Build the dashboard from four core inputs. Clinical leaders should report on AI tools that touch care pathways, along with any patient safety events. IT and security teams should provide model inventories, patch status, and incident response readiness. Compliance and privacy officers should flag open HIPAA findings and data-use approvals. Legal and risk management should summarize vendor contract protections and any liability exposure. From there, pull in outputs from governance, risk, privacy, vendor, and incident review. A central AI governance committee should combine those inputs into one board view. And these same metrics should feed the operating workflow, not just sit in a slide deck.
The table below shows the KPIs and KRIs that belong in a board-ready healthcare AI dashboard, along with how each can be measured in practice:
| Metric Type | Example Metric | How to Measure |
|---|---|---|
| KPI – Program maturity | % of AI use cases with approved governance documentation | AI use case inventory vs. completed governance dossiers |
| KPI – Clinical validation | % of AI systems validated before go-live | Change management logs, clinical validation records |
| KRI – Safety exposure | AI-related safety events or near misses per quarter | Incident management system, patient safety reporting |
| KRI – Security posture | AI systems or connected software with overdue security updates | Vulnerability management platform, vendor patch logs |
| KRI – Compliance gaps | Open audit findings related to AI governance or HIPAA | Internal audit tracker, compliance management system |
| KRI – Governance exceptions | AI projects that bypassed standard review | Change management logs, AI governance committee records |
Use a one-page AI Oversight Scorecard that turns technical risk into board-level language: patient outcomes, regulatory exposure, and business goals. That's the bridge between day-to-day oversight work and the decisions board members need to make. It also ties together the full scope of this series - governance, risk, privacy, vendor, and incident review - without forcing directors to decode technical detail on the fly.
AHA guidance also suggests that boards consider a dedicated AI or AI/cybersecurity subcommittee so this reporting gets focused attention.[16]
With oversight reporting in place, the next step is turning it into routine control.
7. Putting AI Oversight Into Practice With Censinet AI™
A dashboard is only as good as the workflow data behind it. If that data goes stale, the dashboard does too. Censinet AI™ helps make governance part of day-to-day work by turning approved AI use cases, risk limits, and workflow rules into standard assessments, automated vendor reviews, and dashboards that match the organization’s governance model.
The first step is a complete AI inventory. Censinet AI Telemetry classifies inventory items as AI-enabled, not AI-enabled, or unknown, which gives teams a dependable starting point for oversight.[4] Once that inventory is in place, the platform converts each use case - whether it’s a sepsis model, documentation assistant, or revenue-cycle tool - into a standard review. That review looks at model origin, PHI exposure, bias testing, explainability, and alignment with NIST AI RMF and HIPAA requirements.
After the review, the system routes the request, tracks approvals, and keeps the audit trail intact. If a department submits a request for a new AI tool, Censinet AI™ can send it to security, privacy, compliance, clinical leaders, and supply chain for review. Every approval or exception is logged, so teams have a traceable audit record instead of a mess of email threads and side conversations.
The table below maps the main risk domains healthcare organizations should focus on to the oversight artifacts Censinet AI™ helps produce:
| Risk Domain | Oversight Focus | Artifact or Output |
|---|---|---|
| Clinical Safety | Diagnosis support, triage, and predictive analytics | Clinical validation records, risk assessment reports |
| Privacy & Data Use | PHI in model training, prompts, and outputs | Data use approvals, HIPAA compliance documentation |
| Cybersecurity | EHR integrations, model poisoning, prompt injection | AI Telemetry reports, automated vulnerability assessments |
| Vendor | Shadow IT, BAAs, subcontractor exposure | Vendor risk scores, BAA and contract review records |
| Governance | Policy adherence, board accountability, NIST AI RMF alignment | AI inventory reports, board-ready dashboards |
For organizations that are just getting started, it makes sense to roll this out in phases. Begin with the highest-risk or highest-volume AI use cases, build intake and assessment workflows in the platform, and then extend that same process across departments and vendors.
Table: Ad Hoc AI Experimentation vs. a Formal AI Governance Program
One number makes the gap hard to ignore: 51% of healthcare organizations rely on ad hoc discovery to identify AI products in use, and more than 90% lack automated AI product monitoring[18]. That’s not a small process issue. It means many teams are using AI without a clear system for seeing what’s in play, who owns it, or where risk may be building.
This table pulls the main themes together: governance, risk, privacy, vendor review, incident response, and board oversight. It gives leaders a simple side-by-side view of how ad hoc AI use differs from a formal program.
| Dimension | Ad Hoc AI Experimentation | Formal AI Governance Program |
|---|---|---|
| Accountability | Decisions sit in departments; accountability is diffuse. | Named committee and sponsor own review and reporting. |
| Tool Inventory | No central registry exists; AI tools enter through untracked purchases, embedded features, or internal builds. | Single registry tracks tools, models, features, owners, and risk tier. |
| Approval Process | Reviews are inconsistent or skipped. | Standard intake routes tools through security, privacy, compliance, legal, and clinical review. |
| Risk Visibility | Risk is reactive; issues surface after an incident or audit, with limited visibility into PHI exposure, drift, or regulatory gaps. | AI-specific risk registers and dashboards give executives and the board a clear view of risk posture and trends. |
| Escalation Paths | Problems move through informal channels; AI incidents may be treated as generic technical issues. | Defined escalation paths and playbooks route issues to the right teams for triage and containment. |
| Policy Ownership | AI use falls under general IT or data policies, with unclear ownership and no lifecycle provisions. | AI-specific policies have clear owners, review cycles, and alignment with HIPAA, FDA guidance, state privacy laws, and internal standards. |
| Monitoring | One-time checks; no routine drift, bias, or security tracking. | Continuous monitoring with thresholds, alerts, and revalidation. |
The pattern shows up in every row. Ad hoc experimentation reacts after something goes wrong. A formal governance program builds review, oversight, and monitoring into the process from the start. One approach waits for trouble. The other is built to spot issues before they reach patients, regulators, or the board.
Use this baseline to map NIST AI RMF categories to specific healthcare AI use cases.
Table: NIST AI RMF Checkpoints Mapped to Healthcare AI Use Cases
These seven review points give teams a practical way to test each AI use case. For tools that shape clinical decisions, the bar should be higher. The goal is simple: turn governance policy into a repeatable review that clinical, security, compliance, and operations teams can use every time a new AI system comes in.
Use the prompts below during governance review.
| NIST AI RMF Checkpoint | Imaging AI | Ambient Documentation | Revenue Cycle Automation | Patient Triage AI | Cybersecurity AI |
|---|---|---|---|---|---|
| Validity | Validated on our population and scanner types, with subgroup sensitivity/specificity? | Validated against clinician notes across specialties? | Trained on current codes and payer rules, with no systematic coding bias? | Validated on our ED population - age, race, comorbidity mix - with performance and calibration data? | Tuned for healthcare-specific traffic patterns, distinguishing normal clinical behavior from real threats? |
| Reliability | Performance consistent across sites, image quality levels, and scanners, with drift monitoring? | Consistent across accents, background noise, telehealth visits, and documentation styles? | Consistent across payers and service lines as payer policies change? | Performance tracked by shift, census level, and site, with revalidation after major workflow changes? | Alert and true-positive rates stable over time and across campuses, with false-positive fatigue monitored? |
| Safety | AI suggestions treated as decision support, not autonomous diagnosis, with escalation paths for missed or incorrect flags? | Near misses - wrong medication or incorrect diagnosis in a generated note - captured and reviewed as safety events? | AI-driven prior authorization workflows reviewed for delays or inequities in patient access? | Human-in-the-loop controls in place for triage scores, with adverse events tracked by triage category? | Impact of automated containment on critical clinical systems assessed, with tested playbooks to avoid disrupting EHR or PACS? |
| Security | DICOM images and model endpoints protected with access controls, network segmentation, and anomalous-query monitoring? | Audio streaming encrypted in transit and at rest, recordings stored or deleted per policy, and vendor API security auditable? | Claims and financial data protected against ransomware and fraud, with monitoring for billing logic manipulation? | Triage interfaces protected within the clinical network, with model endpoints shielded against adversarial inputs? | AI platform meets healthcare security requirements, with hardened infrastructure and integration into existing SIEM/SOC practices? |
| Explainability | Heatmaps, saliency overlays, or structured rationales available for legal review? | Clinicians can see which transcript elements drove specific problem lists, assessments, or plans? | Finance and compliance teams can see why the AI recommended a code or denial prediction, with auditable rationales? | Risk factors driving a triage score visible to clinicians in a way that supports - rather than replaces - clinical judgment? | Security leaders can explain why an alert fired and communicate those reasons to clinical stakeholders when workflows are affected? |
| Privacy | Images de-identified where possible, with a data use agreement specifying vendor retention and PHI use? | Vendor signs a HIPAA-compliant BAA, limits secondary PHI use, and avoids training global models on identifiable patient conversations? | Vendor limits secondary use of patient and guarantor data and complies with HIPAA and applicable state privacy laws? | Triage data - including social determinants and behavioral health information - handled under HIPAA minimum necessary standards? | Monitoring of user behavior and system logs balanced with workforce privacy, with PHI in logs properly minimized? |
| Accountability | Named owner - such as a radiology service line leader - responsible for approving indications, monitoring dashboards, and responding to AI-related incident reports? | Use-case approval owned by specialty, with documentation quality metrics tracked and reported to clinical governance? | Clear ownership between revenue cycle, compliance, and legal for approving configurations, monitoring denial trends, and responding to payer or regulator inquiries? | Designated clinical governance group reviews outcome metrics - time-to-provider, adverse events by triage category - and approves threshold or deployment changes? | Clear authority for who authorizes automated response policies, who can override them, and how AI-driven incidents are reviewed by risk and compliance? |
The results should feed directly into intake, approval, and monitoring in the next webinar session. And this part matters: answers need proof behind them, not gut feel. That means performance data, BAAs, drift logs, incident reports, and named owners.[19]
If a leader can’t point to that proof for a given system, treat that gap as a risk-register item.
Table: Standard Vendor Due Diligence vs. AI-Specific Vendor Review
Turn the vendor-risk questions from the previous session into a simple pass/fail procurement checklist with this table. The key idea is plain: AI vendor review goes beyond standard procurement. It adds checks for training data, model changes, and clinical or day-to-day decision risk.
This review should be done as a group. That means procurement, legal, compliance, security, and clinical owners all need to look at the same checklist together.
| Review Area | Standard Vendor Due Diligence | AI-Specific Vendor Review |
|---|---|---|
| Security Controls | Encryption, access controls, SOC 2 or HITRUST attestation, breach history | AI hardening and prompt-injection controls |
| Privacy & HIPAA | BAA in place, PHI safeguards, minimum necessary standards | PHI training limits, de-identification validation, and expert-determination documentation [20] |
| Training Data | Usually omitted | Data lineage, source disclosure, de-identification method, and use-rights limits |
| Model Transparency | Architecture overview, feature documentation | Model cards, intended use, failure modes, confidence behavior, and explainability |
| Bias Testing | Usually omitted | Subgroup performance, fairness metrics, and mitigation steps |
| Change Management | Patch management, versioning, release notes | Retraining triggers, pre-release validation, rollback, and change notice |
| Embedded AI Disclosure | Usually omitted | Third-party AI components, open-source dependencies, and upstream model providers |
| Fourth-Party Exposure | Subcontractor list, general security requirements | Subprocessor data flows, hosting locations, upstream PHI handling, and subcontractor training limits |
| Contractual Data-Use Limits | Data retention, return at termination, general confidentiality | Cross-customer training limits, secondary PHI-use limits, reidentification bans, and incident notice timelines |
| Ongoing Monitoring | Uptime, availability, SLA compliance | AI telemetry, drift detection, output-quality monitoring, and escalation contacts |
Use the right-hand column as a go/no-go gate. No AI vendor should move forward unless both the standard controls and the AI-specific controls pass.
If there’s a gap in the AI review column, treat it as a problem to fix before go-live. In practice, that means it moves into incident response and contract management first.
Table: AI Incident Types, Response Teams, and Evidence Requirements
Even after go-live, AI risk doesn’t disappear. It just moves from buying and setup into response. And that matters, because governance only means much if it still holds up when something goes wrong.
A lot of AI incidents don’t look like classic outages at first. They often show up as workflow problems or patient-safety issues. For example, a clinical decision support tool might steer clinicians toward the wrong next step without setting off an obvious alert. That’s why AI incidents need their own taxonomy. But they should still move through the incident process you already use. In practice, that means using the same playbook your team uses for cyber, privacy, and patient-safety events.
The table below links five common AI incident types to response owners, regulatory and clinical timelines, and the evidence teams should collect. Think of it as an extension of your current security, privacy, and patient-safety workflows.
| AI Incident Type | Primary Response Owner | Supporting Teams | Key Response Timeframes | Evidence for Review and Reporting |
|---|---|---|---|---|
| AI-Enabled Device Malfunction | Clinical Engineering / Biomedical Engineering + CMIO | IT Infrastructure, Quality & Patient Safety, Risk Management, Device Vendor | Triage within 2–4 hrs; containment within 24 hrs for high-risk events; user-facility death reporting within 10 working days; manufacturer MDR filing within 30 days for serious injury or death[22][23] | Device logs, error codes, software/firmware version, input/output samples, change records, vendor field service reports, safety event documentation |
| Unsafe Clinical Recommendation | CMIO / CDS Governance Committee | Pharmacy, Nursing, Quality, Patient Safety, Data Science, Ethics (if harm occurred) | Clinician feedback review within 24–72 hrs; disable high-risk pathways within 24–72 hrs of confirmation; root cause analysis within 1–4 weeks | CDS logs (inputs, outputs, model scores), clinical guidelines showing deviation, user interaction logs, override rates, safety/quality reports, governance approval records |
| PHI Exposure in AI Workflow | HIPAA Privacy Officer | Information Security/CISO, Data Governance, IT Operations, Legal | Technical containment within 24–72 hrs; HIPAA breach notification to HHS OCR and affected individuals no later than 60 days after discovery for breaches of 500+ records; smaller breaches logged and reported annually[21][24][25] | Data flow diagrams, access logs, PHI type and volume, BAAs and data-use agreements, privacy risk assessment, de-identification validation records |
| Adversarial Inputs / Prompt Manipulation | CISO / SOC | AI Engineering, IT Operations, Application Owners | Near-real-time detection via SOC; security analysis within hours; interim controls within hours to a few days | Exact prompts or adversarial inputs, model response logs, system prompt settings, guardrail trigger records, security telemetry (IPs, timing, usage patterns), post-incident replication test results |
| AI-Driven Phishing / Social Engineering | CISO + Security Awareness Function | IT Help Desk, HR, Communications | Detection within minutes to hours; account lockouts and MFA enforcement within hours; full campaign analysis over days to weeks | Phishing message copies (email/SMS/voice), headers and metadata, authentication and access logs, email gateway and EDR alerts, user reports, help-desk tickets |
One signal deserves close attention: clinician override rates. If override rates get too low, that can point to overreliance, which can turn into a patient-safety problem.[23] It’s smart to wire these deadlines straight into incident runbooks and on-call escalation so teams aren’t figuring them out in the middle of an event.
Table: Sample Board AI KPIs and KRIs
These are the quarterly metrics that turn AI governance into board-level oversight. KPIs help track adoption and completion. KRIs show unresolved risk and overdue fixes. Put together, they show both how fast AI is moving and whether controls are doing their job.
| Metric Category | Sample KPI / KRI | Type | Escalation Threshold |
|---|---|---|---|
| AI Tool Inventory | AI tools approved, under review, or paused, by risk tier and use case (clinical, operational, patient-facing, security) | KPI | Pause new approvals if more than half the inventory is still under review |
| Vendor Oversight | % of AI vendors with completed security, privacy, and clinical safety assessments; % with annual reassessments up to date | KPI | Escalation required if fewer than 90% of active AI vendors have a completed assessment |
| Incident Management | AI incidents opened vs. closed; mean time to resolution (MTTR) by severity | KRI | Brief the board immediately if any High or Critical incident stays open beyond 48 hours |
| High-Risk Findings | # of outstanding critical and high findings; # of critical clinical workflows that depend on high-risk vendors | KRI | Escalation to CEO/Board if high-risk remediation exceeds 30 days; board review if >10% of vendors have overdue high-risk findings |
| Training Completion | Clinician, nursing, IT, and security staff AI training completion rates by role and service line | KPI | Require retraining if clinical completion drops below 95% |
| Remediation Aging | Open findings by age: 0–30, 31–90, 91–180, and over 180 days; % of critical/high findings past target closure date | KRI | Board-level review if any critical finding exceeds 60 days open without a documented remediation plan |
Two metrics tend to tell you a lot, fast: remediation aging and role-based training completion. They show whether governance is alive in day-to-day work, not just sitting in a policy binder.
This setup works best when the numbers come from one governed record, not a pile of separate spreadsheets. Use RiskOps to pull inventory, vendor status, open findings, incident data, and training completion into a single board dashboard.
Conclusion: Turning AI Enthusiasm Into Disciplined Oversight
AI matters. The issue now is whether leaders can govern it safely across clinical workflows, vendor relationships, patient data, and regulatory duties before an incident forces action. The rest of this series turns that challenge into day-to-day practice.
This series gives leaders a repeatable path from policy to execution. Taken together, it shows how to evaluate, approve, monitor, and respond to AI in a consistent way.
That kind of shift only sticks when clinical, IT, security, and compliance teams work from the same policies, intake process, and data. Without that shared model, intake, review, and monitoring tend to drift and become inconsistent.
Once the process is in place, the last step is support at the workflow level. Censinet can centralize intake, evidence, vendor review, and reporting in one workflow, so automation helps human review instead of taking its place.
Executives who move now will be in a much better position to protect patients and get more from AI at the business level. The next step is simple: catalog AI use, assign governance owners, and enforce a single review path.
FAQs
How can a hospital start AI governance quickly?
Start with five to seven core principles such as safety, transparency, and accountability. Get board approval for those principles within three months. That gives the organization a clear line in the sand before AI tools spread across teams.
Next, set up a governance committee with eight to twelve members. Include people from clinical care, IT security, and legal. You want the folks who understand patient impact, system risk, and compliance at the same table.
Use a standardized risk-management rubric to review AI projects in a consistent way. That rubric should look at:
- Cybersecurity
- Ethics
- Clinical impact
For smaller organizations, a separate AI committee may not make sense. In that case, AI oversight can sit inside an existing clinical quality or IT governance committee.
Which AI tools should be reviewed first?
Start with one central inventory of every AI tool your organization uses. Put high-risk vendors and tools at the top of the list for quarterly risk reviews. Lower-risk assets can usually be checked once a year.
Pay close attention to AI-enabled systems that influence clinical decisions, process patient data, or were rolled out without formal approval (shadow AI). For vendor reviews, standard frameworks such as HSCC’s third-party AI risk guidelines can give teams a clear way to assess risk.
What should boards track to oversee healthcare AI?
Boards need to keep a close eye on whether AI work lines up with the organization’s mission, values, and business goals. That means more than checking progress on a dashboard. It also means watching how the organization handles risk, including ethical concerns, HIPAA and FDA compliance, reputational risk, workforce impact, and communication with stakeholders.
Boards should also review AI inventories, project status, spending levels, and performance metrics - ideally every quarter. That cadence helps support accountability across the full AI lifecycle, from procurement to decommissioning.
