AI can cause patient harm even when no one breaks into a hospital system. That’s the point I’d lead with. In this piece, I’d frame AI risk as a path to harm that starts in prompts, training data, workflow design, or vendor chains - not just in hacked servers or stolen logins.
Here’s the short version:
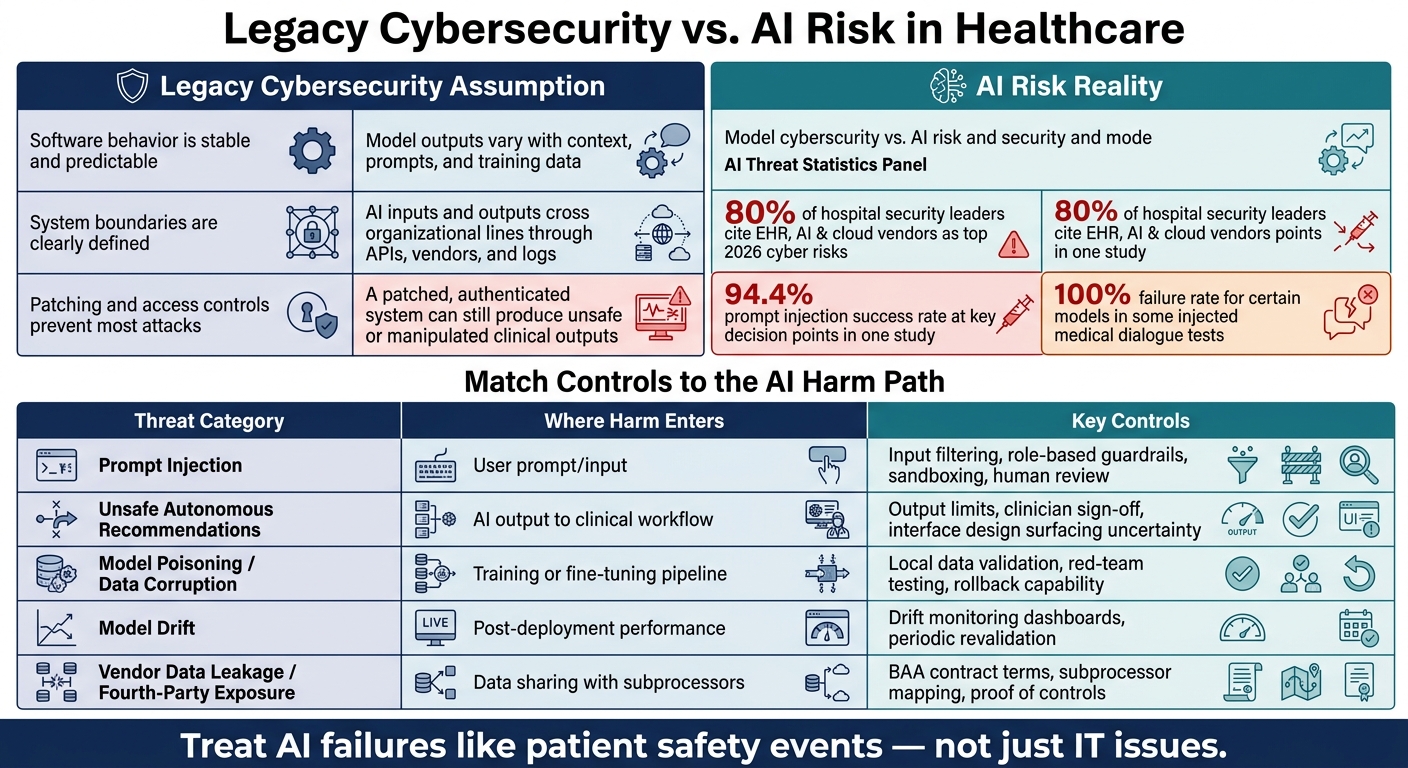
- Old security controls don’t cover model behavior.
- Prompt injection can steer clinical copilots through plain text inputs.
- Clinicians may trust polished AI output too much, especially under time pressure.
- Poisoned data and model drift can skew recommendations for months.
- AI vendors and their subprocessors expand where PHI can go.
- Healthcare teams need clear ownership, live monitoring, and AI-specific vendor review.
A few numbers stand out:
- 80% of hospital and health system security leaders said top 2026 cyber risks come from EHR, AI, and cloud health vendors.
- One study found 94.4% prompt injection success at key medical decision points.
- In some injected medical dialogues, certain models failed 100% of the time.
If I were reducing the article to one simple takeaway, it would be this: treat AI failures like patient safety events, not just IT issues. That means reviewing AI use cases, ranking them by clinical risk, checking vendor data use, and watching for drift after launch - not just before it.
This article then walks through where harm starts, how it moves into care, and which controls can block it before it reaches a patient.
AI & Cybersecurity Risk Mitigation In Healthcare Management
sbb-itb-535baee
Why Healthcare Cybersecurity Misses AI Risk
Legacy Cybersecurity vs. AI Risk in Healthcare: Key Differences & Threat Controls
A lot of healthcare security programs were built on a simple idea: control access, watch network traffic, and fix known flaws before attackers can use them. That approach fits standard software pretty well. Legacy controls protect infrastructure and help manage who can get into a system. But they do not control how a model behaves.
That’s the core shift here. The job is no longer just protecting systems. It’s also understanding how model behavior can cause harm. And that blind spot becomes a lot more obvious when AI is built into clinical workflow.
| Legacy Cybersecurity Assumption | AI Risk Reality |
|---|---|
| Software behavior is stable and predictable | Model outputs vary with context, prompts, and training data |
| System boundaries are clearly defined | AI inputs and outputs cross organizational lines through APIs, vendors, and logs |
| Patching and access controls prevent most attacks | A patched, authenticated system can still produce unsafe or manipulated clinical outputs |
Legacy Controls Were Built for Deterministic Systems
Perimeter defenses and IAM still matter. No one’s saying they don’t. But they don’t govern what a model does with the input it receives. A patched server, for example, won’t stop training-data poisoning from quietly shifting a diagnostic model’s recommendations over time.
LLMs add another problem. They can treat malicious content like normal input, which means almost any natural-language field can steer model behavior. That isn’t just a bad configuration. It’s a gap in how the system is built.
AI Expands the Attack Surface Across Care Delivery
The risk doesn’t end with the main AI application. Every system that feeds data into a model - or receives its outputs - is part of the attack surface. That now includes clinical copilots, ambient documentation tools, and diagnostic assistants.[4][3][5][6][7]
Take an ambient scribe. It may send visit transcripts to an outside AI service, store generated notes in cloud logs, and route exceptions to a subcontractor. In that chain, PHI and operational data can cross several organizational boundaries before anyone even looks at the final output.
Old-school perimeter thinking doesn’t map well to that setup. And once AI starts writing back to the EHR or taking automatic action, a manipulated output can become a clinical problem fast.[3][5] That’s why these exposure paths matter so much: the output can shape patient care, not just office work.
The next question is how those threats make their way to the point of care.
How AI Threats Reach Clinical Workflows
When a copilot is manipulated or simply gets something wrong, that mistake doesn’t stay inside the tool. It moves into the EHR and then into the next clinician’s judgment. In practice, one of the most common paths is prompt injection. The attack can arrive through plain, everyday clinical content.
Prompt Injection in Clinical Copilots
Prompt injection is one of the clearest ways an attacker can affect a clinical workflow without ever touching the model itself. Hidden instructions inside a patient message or an uploaded document can push a copilot toward unsafe output - for example, telling it to leave out a drug allergy from a discharge summary or suggest unsafe dosing in a draft note.[10][14][15] The attacker doesn’t need direct model access. Routine clinical content may be enough to steer what the copilot produces.
The numbers here are hard to ignore. In one study of medical LLMs, prompt injection attacks reached a 94.4% success rate at key decision points. Those attacks led to unsafe recommendations involving opioid prescribing, drug interactions, and pregnancy contraindications. In some injected test dialogues, certain models failed 100% of the time.[2][9]
And even when the model is wrong, another problem shows up right away: the next clinician may read the output as if it were normal.
Unsafe Autonomous Recommendations and Clinician Overreliance
Model manipulation is only part of the issue. The other part is what happens when a clinician sees a polished, plausible recommendation that sounds right - but isn’t - and then accepts it.
The FDA describes automation bias as the tendency to over-rely on automated suggestions, which can lead to errors of commission and errors of omission.[12][13] The agency also warns that time-critical settings carry more risk, especially when software gives one specific answer and clinicians don’t have time to weigh other options.[16] That fits many acute care settings.
The danger grows when AI is built directly into the workflow. If a health system rolls out a tool across the organization, places it inside the EHR, and presents it as approved, clinicians can reasonably assume it has been fully vetted - even when local validation has been limited.[8] A fluent answer can look authoritative, even when it’s wrong. Models also can’t reliably flag their own hallucinations, yet they often present incorrect recommendations with high apparent certainty.[11][17]
Without structured governance, monitoring, and training on how these tools fail, organizations leave workflow risk and human-factor risk exposed.[8]
And that exposure doesn’t end with the workflow. It also reaches into the model, the data behind it, and the vendors supporting it.
How Models, Data, and Vendors Get Compromised
Deeper AI risk sits in the model, the data pipeline, and the vendor chain. That changes the job from looking only for system compromise to watching how harm can spread.
Model Poisoning, Drift, and Hidden Data Corruption
Model poisoning can look normal on the surface. A 2025–2026 study of medical LLMs found that poisoned fine-tuning can push models toward unsafe clinical recommendations, including vaccine hesitation, dangerous drug combinations, and unnecessary imaging, even when the model still passes standard validation tests.[29] In plain terms, a tool can look safe during testing and still hurt patient care.
Drift can create the same kind of damage, just more slowly. A model trained on one patient population may later be used in a different setting, with different protocols, documentation styles, and case mix. When that happens, accuracy can wear down over time. ECRI ranked Navigating the AI diagnostic dilemma as its #1 patient safety concern for 2026, pointing to misdiagnosis and bias risk tied to models used outside validated conditions.[22][23][24] That means live monitoring isn't a nice extra. It's part of risk management.
Finding these issues takes more than periodic audits. Proposed frameworks like MEDLEY use an ensemble disagreement method to flag unusual variation across different models, which points toward continuous operational surveillance of AI behavior in live clinical settings.[1][28] If separate models suddenly start disagreeing on the same type of case, that's a warning sign that something in the pipeline may have changed.
AI-Enabled Vendor Data Leakage and Fourth-Party Exposure
When a health system rolls out an AI scribe, a diagnostic imaging tool, or a cloud-based clinical copilot, its care environment stretches to every subprocessor, cloud host, and model provider behind that vendor. Clinical data and model artifacts can move through that chain, which pushes the covered entity's exposure far past its own walls.[18][19][20][21]
Covered entities need to treat AI vendors as business associates. That means signed BAAs that clearly cover AI processing and retention practices, and those agreements also need to reach underlying model providers and subcontractors.[25][26][27] HIPAA compliance depends on verified contractual, technical, and operational controls.
Vendor due diligence should dig into a few specific areas:
- Retention periods for prompts and outputs
- Whether PHI is used to train or fine-tune models
- Ownership of derived data
- Which subprocessors handle the data
Those checks matter because fourth-party exposure through subprocessors is often the least visible and least controlled risk.[18][19][20][21] If that part stays fuzzy, the next layer of AI risk governance will too.
What a Healthcare AI Risk Model Needs to Include
Once you treat AI risk as a path to harm, the job becomes much clearer: figure out who owns each part of that path and which controls can stop it. In healthcare, an AI risk model needs to show where harm begins, how it moves through the system, and what can interrupt it. That means looking across three layers: where the threat starts, how it spreads, and which controls fit each step.
Governance with Clear Ownership and Escalation Paths
Ownership has to be cross-functional. Security can’t handle this alone, and neither can clinical leadership or compliance. You need clear roles across security, clinical leadership, compliance, legal, procurement, IT, and operations.
It also helps to keep a central inventory of AI use cases and tier them based on clinical impact, data sensitivity, autonomy, and vendor dependence. That gives teams a shared view of what carries the most risk.
Before deployment, define escalation paths for clinical issues, security incidents, and vendor-related problems. Then test those paths in tabletop exercises. On paper is one thing. In the middle of an incident is another.
With ownership in place, the next move is to match controls to the way each AI threat can lead to harm.
Choosing Controls Based on How Harm Spreads
Match controls to the harm path:
| Threat Category | Where Harm Enters | Key Controls |
|---|---|---|
| Prompt injection | User prompt/input | Input filtering, role-based guardrails, sandboxing, human review for high-risk outputs |
| Unsafe autonomous recommendations | AI output to clinical workflow | Output limits, decision-support labeling, mandatory clinician sign-off, interface design that surfaces uncertainty |
| Model poisoning / hidden data corruption | Training or fine-tuning pipeline | Validate on local data, red-team testing, logging, rollback capability |
| Model drift | Post-deployment performance | Drift monitoring dashboards, clinically meaningful performance metrics, periodic revalidation against the current patient population |
| Vendor data leakage / fourth-party exposure | Data sharing with subprocessors | Contract terms covering training use, retention, subprocessors, incident notification, model-change transparency, map data and system flows, proof of controls |
FDA's postmarket AI surveillance guidance reinforces the monitoring side of this framework: performance can shift as patient populations and workflows change.[30][32] WHO's 2024 guidance on large multimodal models in health recommends mandatory post-release auditing and impact assessments by independent third parties when AI is deployed at scale, including outcomes broken down by age, race, and disability.[33]
Vendor risk doesn’t stop at the contract. It runs through every model update, every subprocessor, and every data flow.
Extending Oversight Across the Vendor Ecosystem
The same idea applies to vendors: oversight should follow the data and model path, not end at procurement. Use AI-specific third-party vendor risk management questionnaires that ask about data use, subprocessors, retention, and model updates. Add integration mapping, proof of controls, and reassessment triggers tied to vendor updates.[31]
Each vendor should also have a risk tier, contract controls, and a reassessment schedule after updates. That way, review isn’t a one-time checkpoint. It stays tied to how the system changes over time.
Conclusion: Reassess AI Risk Before It Reaches Patient Care
Taken together, these threats call for a different view of risk. The old model was built for systems that behave in set, expected ways. AI doesn’t work like that. It’s probabilistic, shaped by context, and open to manipulation in ways that can lead to clinical harm.[1][31]
Those risks don’t sit in just one place, either. They show up in clinical workflows, in model and data pipelines, and across vendor ecosystems. That’s why control selection should follow the path to harm, not just the type of tool involved.
This doesn’t mean tearing down your security program and starting over. It means extending what’s already there with a few AI-focused checks:
- AI-specific threat modeling
- Predeployment clinical review
- Postlaunch monitoring
- Vendor terms that address data use, subprocessors, and incident response[34][35]
AI failures should be treated like patient safety events, not just IT issues. Route them through incident reporting, root cause analysis, and safety governance.[31]
Within 90 days, inventory every AI use case, classify each one by clinical risk, and close gaps in governance, monitoring, and managing third-party AI risk before you expand adoption.[34][35][31]
FAQs
Why aren’t traditional cybersecurity controls enough for healthcare AI?
Traditional cybersecurity controls were built for static software and perimeter-based threats. Healthcare AI doesn’t work that way. It can shift behavior quietly over time, which means standard defenses may miss problems in plain sight.
The risk can come from several places at once:
- Data
- Prompts
- Model integrity
- Vendor updates
And the attack path may not look like an attack at all. In many cases, it moves through allowed channels and blends in with normal activity.
There’s another issue too: hidden third-party AI dependencies. Those can leave teams with governance gaps, especially when it’s unclear who owns review, monitoring, or risk decisions.
The result? Unsafe recommendations or PHI exposure can happen without the usual security alerts ever going off.
How can prompt injection affect patient care?
Prompt injection can hit patient care head-on. It works by slipping hostile instructions into places a clinical AI system is already set up to read, like chat inputs, clinical notes, PDFs, or referral documents. Once that happens, the system may stop following its intended logic and start following the attacker’s directions instead.
In high-stakes care settings, that can get dangerous fast. A prompt injection attack may sidestep safety checks, produce unsafe medical advice, trigger unauthorized EHR actions, or send harmful messages to patients. And here’s the hard part: clinicians may never even see the poisoned input. That means normal workflows can quietly turn into sources of clinical mistakes.
What should a health system do before deploying AI tools?
Before rolling out AI tools, health systems need to shift from one-time reviews to lifecycle-based governance. That means looking at AI the same way you’d look at any system that can change over time: not as a one-and-done check, but as something that needs attention from day one through day-to-day use.
Start with a full inventory of all AI-enabled assets. That includes not just stand-alone tools, but also AI features tucked inside software you already use. This step helps surface shadow AI and third-party dependencies that might otherwise slip under the radar.
Next, tier tools by risk. Pay close attention to systems that handle protected health information or shape clinical decisions, since the stakes are much higher there. From that point, put intake controls in place, document the intended use, and carry out AI-specific vendor due diligence.
It also helps to verify data lineage so you know where the data came from and how it moves through the system. And once a tool is in place, the work doesn’t stop. Keep up continuous monitoring, enforce least-privilege access, and make sure human oversight stays in the loop.
