Healthcare is using AI faster than it is controlling it. In 2024, 71% of hospitals said predictive AI was built into their EHRs, but only 18% had a mature governance setup. My takeaway is simple: if you use AI in care, billing, documentation, or patient messaging, you need one clear system for approval, review, monitoring, and shutdown.
Here’s the short version:
- Put every AI tool in one inventory, including shadow AI
- Assign 3 owners for each tool: clinical, technical, and risk/compliance
- Sort tools by risk, because a sepsis alert is not the same as a billing helper
- Review AI across its whole life cycle, from intake and validation to drift checks and incident response
- Check vendors beyond the BAA, including model limits, subgroup bias, PHI use, and outage reporting
- Map controls to the use case, since chatbots, radiology AI, and ambient scribes create different risks
- Set stop rules before launch, so teams know when to pause or turn a tool off
I’d boil the article down to this: treat healthcare AI like any other high-risk system that can affect patients, data, or compliance. That means local validation, human override, audit logs, clear approval rights, and board-level visibility for high-risk use.
A few facts make the issue hard to ignore:
- Only 22% of hospitals say they could produce a full AI audit trail within 30 days
- More than 90% of healthcare groups lack automated AI product monitoring
- 51% still rely on ad hoc discovery to find AI already in use
- In one review of 903 FDA-approved AI-enabled medical devices, 24.1% said no clinical performance studies were conducted
If I were putting this into action today, I’d start with four steps: inventory every tool, create a governance committee with decision rights, set risk tiers, and require validation plus vendor evidence before go-live. That is the core playbook.
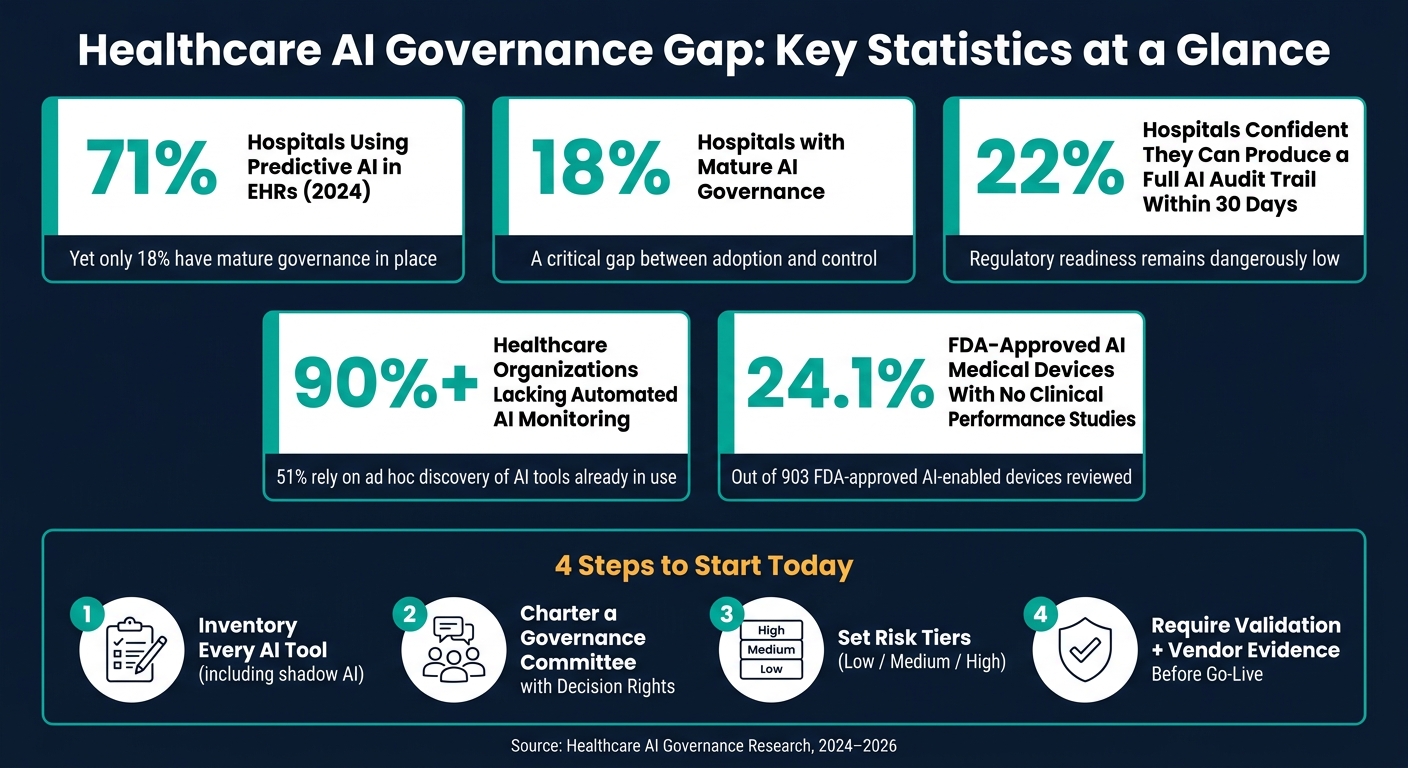
Healthcare AI Governance Gap: Key Statistics at a Glance
Healthcare AI Governance - Risks, Compliance, and Frameworks Explained
sbb-itb-535baee
Build a cross-functional AI governance model with clear accountability
Once the regulatory baseline is clear, the next move is simple: decide who approves AI, who owns it, and who can shut it down.
Set up an AI governance committee and define decision rights
This committee should include executive leadership, the CISO, CIO, CMIO, or Chief AI Officer, plus compliance, privacy, legal, quality, patient safety, clinical leaders, IT/data science, and patient/community representatives.
Its role is to approve new AI use cases, set pilot conditions, define validation standards, set monitoring thresholds, require manual override rights, and own escalation paths when incidents or bias concerns surface.
The key word here is authority. This group needs formal power to approve, change, or decommission tools, not just offer input.
Before go-live, require an evidence package with:
- intended use
- data provenance
- validation results
- monitoring plan
- rollback plan
Roughly 90% of governance friction stems from missing evidence rather than poor model quality [3].
Approval alone doesn’t solve the problem. Every approved system also needs named operational owners.
Assign system-level owners through designated AI ownership
Each production AI system should have three named owners: a clinical owner, a technical owner, and a risk/compliance owner.
- Clinical owner: use aligns with care standards.
- Technical owner: model performance and drift monitoring.
- Risk/compliance owner: access controls, threshold enforcement, and shutdown authority.
This makes inventory work and annual risk review far more practical. Only 22% of hospitals are highly confident they could produce a complete AI audit trail within 30 days for regulators [1].
Ownership only works if every AI system shows up in one inventory.
Build an enterprise AI inventory and risk tiering model
You can’t govern what you haven’t cataloged. Every AI tool should be logged with its use case, PHI exposure, vendor, integrations, data source, and patient risk level, whether IT bought it or a clinical department started using it. That inventory also helps surface shadow AI, including tools used without required BAAs [4].
After that, each tool gets a risk tier. That tier sets the depth of review, the controls required, and how often the tool needs monitoring.
| Risk Tier | Example Use Case | Patient Safety Impact | Review Depth | Required Controls | Monitoring Cadence | Approval Authority |
|---|---|---|---|---|---|---|
| Low | Scheduling optimization, billing automation | Minimal | Standard IT/security review | Standard IT security & BAA | Annual | Department Head / IT |
| Medium | Prior auth summarization, clinical documentation | Moderate | Clinical informatics + privacy review; bias check | Human-in-the-loop; audit logging | Quarterly | Governance Committee |
| High | Radiology diagnostic AI, sepsis alerts, drug dosing | Direct impact on diagnosis/treatment | Full committee + shadow deployment + local validation + PCCP review | Human override; versioning; PCCP | Continuous / real-time | Board / Chief AI Officer |
For high-risk tools, use shadow deployment, or a parallel run, before go-live. Then require local validation. Vendor claims and FDA clearance are not enough. An analysis of 903 FDA-approved AI-enabled medical devices found that 24.1% explicitly stated no clinical performance studies were conducted [1].
Standardize AI risk assessment and controls across the lifecycle
Governance only works when every AI tool goes through the same path from intake to monitoring. That means taking policy decisions and turning them into a repeatable process for intake, review, approval, and follow-up.
Use a healthcare-specific set of AI risk criteria
Generic IT risk checklists don’t catch the kinds of harm that matter in healthcare. A better starting point is FAVES - Fairness, Appropriateness, Validity, Effectiveness, and Safety [5][6]. It gives clinical, legal, and compliance teams a common way to talk about risk. It also lines up well with the NIST AI RMF’s four core functions: Govern, Map, Measure, and Manage.
From there, the review should cover a few key areas.
On the data and privacy side, verify encryption in transit and at rest. Confirm that role-based access controls are in place. And make sure your Business Associate Agreement clearly states whether PHI will be used in training or fine-tuning [5][1].
On the cybersecurity side, look for AI-specific threats, not just standard software issues. That includes prompt injection, data poisoning, adversarial inputs, and PHI leakage. For any AI tool used in a clinical workflow, require a Software Bill of Materials (SBOM) [5][2].
If a tool affects care decisions, clinical validation and explainability need extra attention. Check whether the tool meets the FDA’s definition of Software as a Medical Device (SaMD). Ask the vendor to explain how the model produces its outputs. Also check whether the training data matches your patient population. A model trained mostly on data from urban academic medical centers may not perform well in a rural or safety-net setting [1].
Under ONC HTI-1, developers of predictive decision support tools built into certified EHRs must disclose source attributes, including training data demographics, exclusion criteria, and known limitations. That gives clinical users the context they need to judge outputs more carefully [5].
Those criteria should feed the same workflow every time a team reviews a tool.
Follow a common workflow from intake to approval and monitoring
The workflow should move through the same stages each time: intake, initial screening, risk tiering, domain review, committee approval or conditional approval, pilot with defined controls, production monitoring, and formal reassessment after any material change.
One point matters more than it may seem: pre-deployment validation and post-deployment monitoring are not the same thing. When teams blur those together, gaps show up fast.
| Control Category | Pre-Deployment | Post-Deployment |
|---|---|---|
| Validation | Vendor Model Cards, peer-reviewed studies, shadow deployments | Real-world performance monitoring, local validation audits |
| Data/Privacy | BAA execution, data minimization, encryption setup | Access audits, PHI leakage monitoring, DUA compliance checks |
| Risk Management | Risk tiering, bias impact assessments, SBOM collection | Drift monitoring, reassessment after material changes |
| Human Oversight | Defined decision rights, staff literacy training | Adverse event reporting, human-in-the-loop override logs |
Set stop conditions before go-live. For example, define a false-negative threshold that triggers a pause or shutdown [6]. If you don’t set those triggers upfront, trouble tends to show up after harm has already started.
That risk is far from theoretical. More than 90% of healthcare organizations lack automated AI product monitoring, and 51% rely on ad hoc discovery of AI tools already in use [5].
Use Censinet to centralize AI risk workflows and oversight
Trying to run this process across dozens of AI tools, several departments, and changing governance committee members without a central system is asking for chaos. Documentation ends up in spreadsheets. Approvals disappear into email threads. Monitoring gets uneven.
Censinet RiskOps™ acts as a central hub for this work. It brings AI inventories, risk assessments, governance records, and task routing into one platform, so risk teams have a single source of truth instead of a scattered set of files. Real-time dashboards show where each tool sits in the review cycle, which controls are still pending, and which systems need reassessment.
Censinet AI and Censinet AITM add automation with human review. Teams can speed up evidence review, policy drafting, and risk summary generation without taking people out of the decision process. You can use the platform to send findings and tasks to the right owners while keeping human review in place. Risk teams stay in control through configurable rules and review workflows, so automation supports decisions rather than making them on its own.
These controls should apply to every third-party AI tool before procurement.
Strengthen third-party AI oversight and map use cases to HIPAA controls
Once your internal lifecycle controls are in place, the next job is vendor oversight. That's where a lot of AI risk shows up. Many healthcare teams don't build every AI system themselves - they buy tools, plug in services, or rely on outside platforms. So if a third-party product touches ePHI, a signed BAA is the starting point. But it should never be the whole approval process.
Evaluate AI vendors with security, privacy, bias, and resilience checkpoints
The table below shows what should qualify a vendor for approval at onboarding - and what should stop the process.
| Area | Acceptable Vendor Pattern | Unacceptable Vendor Pattern |
|---|---|---|
| BAA & Data Use | Signed BAA; clear restrictions on using customer PHI for model training [4][1] | Refuses to sign BAA; trains models on customer PHI without de-identification [4] |
| Model Transparency | Provides Model Cards or equivalent; discloses training data demographics, known limitations, and validation results; includes a PCCP for adaptive algorithms [4][1] | Undocumented models; no disclosure on training data or limitations [1] |
| Incident Notification | 24-hour incident reporting commitment [2][4] | No formal notification process for model drift, security incidents, or service disruptions [4] |
| Business Continuity | Documented continuity for AI-enabled workflows [2][4] | No continuity plan for AI-dependent clinical or operational processes [4] |
A security review matters, but it won't tell you everything. It can show whether a vendor uses encryption, access controls, and incident response. What it won't show on its own is whether the model performs unevenly across patient groups.
HHS OCR Section 1557 requires disparity review across patient subgroups. That means vendor review has to include bias testing before deployment and audits after launch. Without that step, it's easy to miss harm that hides behind decent security paperwork.
A 2019 study made this problem hard to ignore. An algorithm used healthcare costs as a stand-in for health needs and systematically underestimated the illness of Black patients. Fixing that issue required increasing the share of Black patients receiving additional care from 17.7% to 46.5% [1]. That kind of gap won't show up in a standard security questionnaire.
Map common AI use cases to required controls and owners
The same vendor can be fine for one workflow and risky for another. That's why controls need to match the actual use case, not just the product name on the contract. In healthcare, each AI deployment brings its own HIPAA duties and should have a named owner.
| Use Case | HIPAA Safeguards | Governance & Validation Needs | Monitoring Owner |
|---|---|---|---|
| Ambient Clinical Documentation | Access controls; audit controls; BAA [4] | Accuracy review; correction workflows [1] | Clinical Informatics & Compliance |
| Imaging Support (Radiology AI) | Transmission security; integrity [4] | Modality-specific local validation; indication tracking; PCCP review [1][4] | Radiology Dept / Quality Safety |
| Patient Engagement Chatbots | Identity verification; encryption [4] | Escalation to human staff; safe response boundaries; message logging [1] | Patient Experience / IT Security |
Local validation isn't optional. A tool that performs well in a vendor demo may fall short in your hospital, your patient mix, or your workflows. An independent 2026 study of the Epic Sepsis Model found materially lower performance on local data than the developer reported, which reinforces the need for site-specific validation [1].
Use Censinet Connect™ and Censinet AITM to scale vendor assessments

Once the checklist is set, scale becomes the problem. Reviews can slow down fast when every vendor sends different documents in different formats.
Censinet Connect™ helps standardize that intake process with vendor questionnaires and structured evidence exchange. That makes it easier to review the same checkpoints each time, including BAA status, model documentation, training-data restrictions, and incident response duties, instead of sorting through ad hoc submissions that are tough to compare.
Censinet AITM speeds up the review side. It organizes vendor evidence intake so teams can assess documentation in a consistent way, while human reviewers still make the final approval decision through configurable workflows.
Conclusion: A practical operating model for safe, accountable healthcare AI
Healthcare has moved into AI faster than it has built the guardrails around it. The fix isn't complicated, but it does take discipline. Use the same control model already applied to regulated clinical systems. In practice, that means one clear setup: defined ownership, a full inventory, and risk tiers that decide which controls apply to which tools.
AI governance also can't sit with one team and call it a day. Providers, vendors, and device makers all have a part to play. So the process needs to be shared too: one workflow for approvals, monitoring, and escalation. Any third-party AI risk management that touches PHI should have a signed BAA, bias evaluation, local validation, and a named internal owner who is accountable for how it performs over time. Censinet RiskOps™ can help keep policies, findings, and approvals in one workflow.
Key actions healthcare leaders should take next
This only works when leaders make oversight part of the regular rhythm, not a one-time project.
- Audit every AI tool, including shadow AI.
- Charter a governance committee with documented decision rights.
- Define risk tiers that set approval and monitoring depth.
- Require Model Cards, BAAs, and bias evaluation before go-live.
- Track performance, adverse events, and compliance in board reporting.
FAQs
How do we start AI governance quickly?
Start with a 90-day implementation plan.
In the first 30 days, run a full clinical AI inventory. The goal is simple: find every deployed machine learning, generative, and agentic AI model across the organization.
At the same time, set up your governance structure, define risk assessment criteria, and run a gap analysis for HIPAA, security, and medical device standards.
This early work gives you a clear picture of what’s already in use, who owns it, and where the weak spots are. It also helps you address AI-specific risks such as model drift and data poisoning before they turn into patient safety or compliance problems.
Which healthcare AI tools need the strictest oversight?
Healthcare organizations should apply the strictest oversight to Tier 3 tools. These include predictive systems and decision-support interventions that directly shape clinical actions. Put simply, if a tool can influence what happens in patient care, it needs the highest level of review.
Because these tools can affect patient safety, teams should require rigorous pre-production validation, clear transparency documentation, and ongoing performance monitoring. That means checking the tool before launch, documenting how it works and where it may fall short, and then watching its output over time to catch drift or errors.
Tools that process patient records, generate clinical notes, inform treatment recommendations, or support communications also need strict HIPAA safeguards. They should also go through a formal annual risk analysis.
What should we ask AI vendors before approval?
Before you approve an AI vendor, run a structured review. The goal is simple: spot dependencies early and check whether the vendor’s security setup is solid.
Ask for:
- Regulatory status, including whether FDA clearance is needed for Software as a Medical Device
- Model Cards or similar disclosures that cover training data, known limits, and validation
- Proof of drift monitoring, version control, incident response, and compliance with HIPAA, HITRUST, SOC 2, and NIST AI RMF
