A hospital can do many things right and still get hit through a vendor. In 2024, the Change Healthcare attack disrupted billing, pharmacy work, and patient access across the U.S., while exposing data tied to about 1 in 3 Americans. The big lesson is simple: if one outside partner fails, care, cash flow, and HIPAA risk can all get hit at once.
If I boil this article down, here’s what matters most:
- Most healthcare risk now sits outside hospital walls too.
- Third-party and fourth-party vendors are common entry points for ransomware, malware, and remote access abuse.
- Connected medical devices add more weak spots, especially older devices with poor software visibility.
- The damage goes beyond IT: downtime can slow care, claims outages can stall revenue, and breaches can trigger legal and OCR review.
- The fix starts with three steps: tier vendors by risk using third-party risk assessment questions, put clear security terms in contracts, and test outage workarounds before you need them.
A few numbers make the point fast:
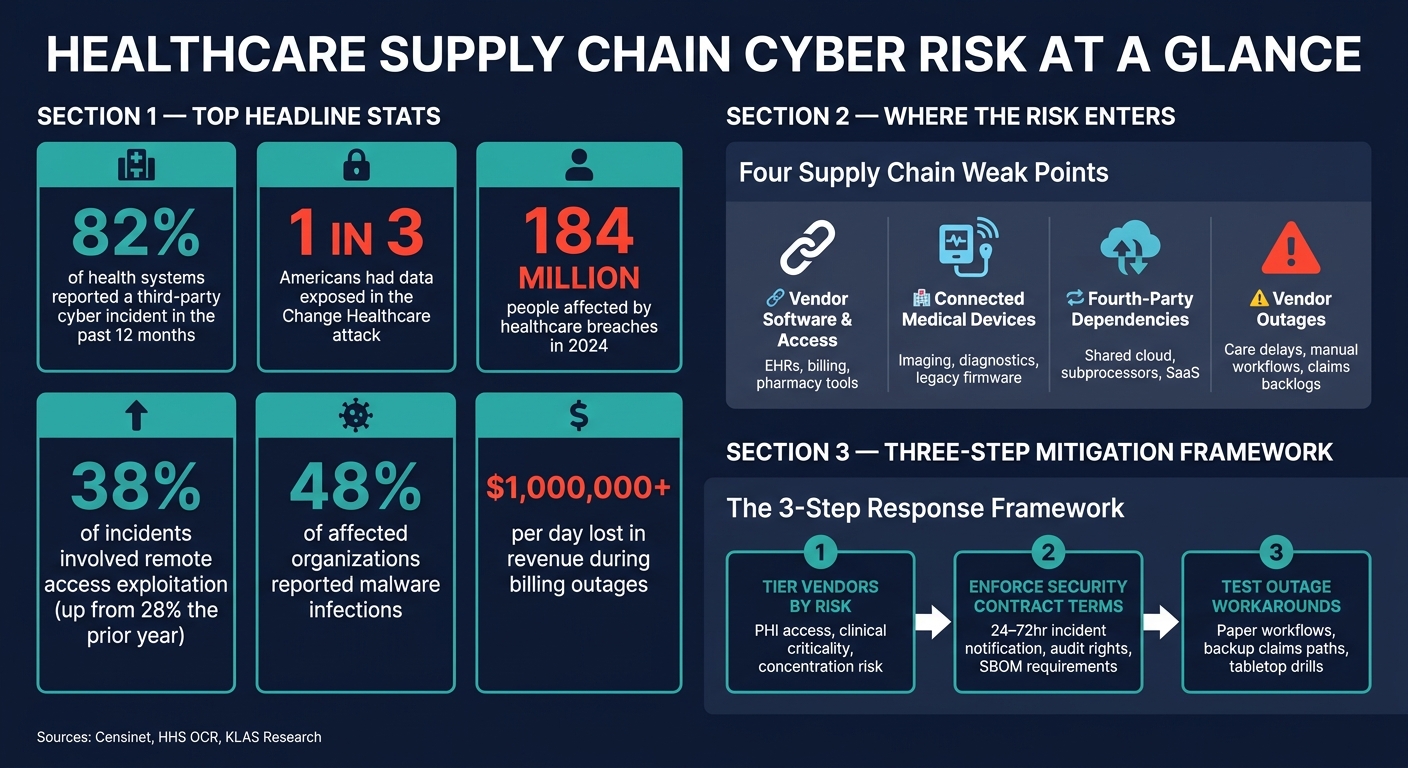
- 82% of health systems reported a third-party cyber incident in the prior 12 months
- 38% of incidents in 2026 involved remote access exploitation, up from 28% in 2025
- 48% of affected groups reported malware infections
- Healthcare breaches in 2024 exposed data for 184 million people
- Some billing outages can cost $1,000,000+ per day in delayed revenue
Here’s the short version of where the risk shows up:
| Risk area | What it can disrupt | What you should focus on |
|---|---|---|
| Vendor software and access | EHRs, billing, pharmacy, support tools | MFA, access review, vendor tiering |
| Medical devices | Imaging, diagnostics, treatment workflows | Asset inventory, firmware tracking, network limits |
| Fourth parties | Shared cloud, subprocessors, SaaS dependencies | Contract disclosure, dependency mapping |
| Vendor outages | Care delays, manual charting, claims backlogs | Paper workflows, backup paths, drills |
My takeaway: supply-chain cyber risk is not just an IT problem. It is a patient care, revenue, and business continuity problem. So if I’m a healthcare leader, I should treat vendor failure the same way I treat internal downtime: as something I need to plan for before it happens.
Healthcare Supply Chain Cyber Risk: Key Stats & Threat Breakdown
How Attackers Reach Hospitals Through the Supply Chain
Third-Party Vendors and Software as Entry Points
Vendor access is often the easiest way in.
Support sessions through VPN, RDP, or Citrix can turn into open doors when MFA is missing. In many cases, all it takes is one phished vendor employee for attackers to get a foothold. From there, they can move into hospital systems through access that already looks trusted.
Software updates can also become a delivery method. Attackers may slip malicious code into trusted updates or third-party libraries before those files go out to customers. That means a routine update can quietly install malware on its own. The Log4j vulnerability is a clear example of software-package compromise at scale. And when hospitals rely on shared service providers like billing platforms or pharmacy processors, one hit can ripple across every organization that depends on them.
Vendor access is only part of the problem. Connected devices open another path.
Connected Medical Devices and Fourth-Party Blind Spots
Many connected medical devices run on embedded software and firmware built with third-party components. Under FDA Section 524B, new devices now require Software Bills of Materials (SBOMs) [2][3]. That gives hospitals more visibility into what sits inside those products.
Older devices are a different story. Many don't have this documentation at all, which leaves security teams in the dark about hidden dependencies and unpatched components.
The problem gets worse when fourth-party risk creates a first-party crisis. A lot of clinical SaaS platforms sit on top of a small group of shared infrastructure providers. So even when a hospital has a contract with one vendor, the actual risk may sit with a subcontractor further down the chain. Security teams often run into these multi-layer dependencies, where the weakest link isn't the company they hired directly [2][1].
Weak points at any supplier tier can expose the whole chain.
Each new clinical tool brings one more outside dependency, and one more opening for compromise.
How Modern Healthcare Expands the Attack Surface
Telehealth, remote patient monitoring, AI-enabled diagnostics, and cloud-based SaaS platforms have increased the number of outside connections health systems rely on. Every new tool tends to bring another vendor, another software dependency, and often another subcontractor working beyond the hospital's direct view.
The numbers show how this is playing out. Remote access exploitation rose to 38% of incidents in 2026, up from 28% in 2025 [3]. Malware infections are still the top attack type, affecting 48% of organizations that experienced an incident [3]. AI is also speeding up the threat side. Automated systems can find vulnerabilities and generate exploits faster than manual patching workflows can keep pace.
"We cannot keep up with patches in a manual fashion, patch by patch at AI speed." - Joe Saunders, CEO, RunSafe Security [3]
| Vulnerability Type | Frequency/Impact | Primary Pathway |
|---|---|---|
| Malware Infections | 48% of incidents | Vendor software/phishing [3] |
| Remote Access Exploitation | 38% of incidents | Management software/VPNs [3] |
| Medical Device Exploit | 80% impact care | Legacy firmware/unpatched components [3] |
| Fourth-Party Failure | Systemic | Subcontractors/shared SaaS platforms [2][1] |
The attack surface keeps growing because modern care now depends on outside systems. And that matters, because a single supplier failure can lead to downtime, lost revenue, and compliance exposure.
sbb-itb-535baee
How Stryker's Cyber Attack Hit Earnings and Hospital Supply Chains #cybernews #stryker #podcast
The Operational, Financial, and Compliance Cost of Supply-Chain Incidents
When attackers get in through the supply chain, the fallout hits operations, revenue, and compliance at the same time. Once a breach reaches a vendor, the clock starts ticking on care delivery, cash flow, and legal risk.
Care Delivery Disruption and Downtime Risk
When a vendor goes down, hospitals feel it almost right away. A cloud EHR outage can push staff back to manual workflows, slow documentation, and even lead to emergency department diversions. If a medical device supplier has a vulnerability, device availability can drop, diagnostic procedures can be delayed, and patient safety can be put at risk.
That’s why downtime planning can’t stop at internal systems. It also needs to cover external vendors. If a key supplier fails, the hospital still has to keep care moving.
Operational damage is just the first hit. Financial loss and legal pressure usually show up next.
Revenue Loss, Response Costs, and Legal Exposure
The money side can spiral fast. A ransomware attack on a billing processor can create claims backlogs and reimbursement delays that cost $1,000,000 or more per day in lost revenue [1]. And that’s just the start. Incident response teams, forensic investigators, and legal counsel all add major costs.
HIPAA accountability still sits with the covered entity, even when a vendor handles the data. A vendor-sourced breach can trigger OCR scrutiny, breach notification duties, and possible class-action lawsuits whether the breach started inside the hospital or outside it. In 2024, healthcare breaches exposed data for 184 million people [1].
Incident Type vs. Business Impact: A Reference Table
The table below shows how three common supply-chain incident types can affect care delivery, cash flow, and compliance.
| Incident Type | Impact on Care Delivery | Impact on Cash Flow | Regulatory & Legal Exposure |
|---|---|---|---|
| Payment Processing Ransomware | Minimal direct clinical impact; delays in elective scheduling. | Severe: Claims backlogs, reimbursement delays, and $1,000,000+ daily revenue loss [1]. | Breach notification obligations; OCR scrutiny of BAAs. |
| Medical Device Supplier Vulnerability | Device unavailability, delayed diagnostic procedures, and patient safety risks. | Replacement or workaround costs. | Potential class-action risk; FDA and regulatory reporting requirements. |
| Cloud EHR Provider Outage | Forced manual workflows, loss of patient history, and emergency department diversion. | Inability to document billable services in real time; delayed coding. | HIPAA compliance and incident response burden. |
The next step is to cut that exposure with continuous vendor risk management and stronger supplier governance.
Supply-Chain Cyber Risk Management: Strategies and Governance for Healthcare
To cut vendor, device, and service-provider risk before the next outage, focus on three controls: tiered assessments, contract terms you can enforce, and fallback plans that have been tested. This has to work in day-to-day operations. Tier suppliers. Put clear terms in contracts. Plan for outages before they hit.
Vendor and Device Risk Assessments and Continuous Monitoring
Start by grouping suppliers based on PHI access, network connectivity, clinical criticality, and concentration risk. Any vendor whose failure could stop billing, medication workflows, imaging, or patient authentication should sit near the top. The same goes for cloud and managed service providers that several internal systems rely on at the same time.
A one-time questionnaire won't do the job. Strong programs pair initial reviews with ongoing evidence checks, such as SOC 2 reports, penetration test summaries, cyber insurance details, and architecture diagrams for critical vendors. They also use continuous monitoring to track shifts in a vendor's internet-facing exposure, new subcontractors, breach activity, and signs of financial or operational distress. Some programs go further and require annual penetration tests plus pre-procurement review of attestations, third-party access, and secure development practices before purchase.[9]
Connected medical devices need a separate lane. Reviews should cover asset inventory, firmware versions, end-of-support dates, and remote service pathways across imaging, medication, registration, and authentication workflows. If patching gets delayed, compensating controls like network segmentation, anomaly detection, and restricted remote access should be documented and watched closely. Put simply: connected-device visibility needs to be part of every vendor risk program.[7][8]
Contract Controls, Supplier Governance, and Recognized Frameworks
Assessment results only matter if contracts turn them into obligations. Critical vendor agreements should require prompt incident notification within 24 to 72 hours, disclosure of major changes in hosting, ownership, or subprocessors, set timeframes for vulnerability remediation, audit rights, and cooperation during investigations. For software vendors, healthcare buyers are also asking for a Software Bill of Materials (SBOM) so they can see component dependencies and known vulnerabilities more clearly.
Ownership should be clear across procurement, security, legal, compliance, clinical engineering, and IT operations, with a business owner assigned to each critical supplier. Material findings - especially anything tied to patient safety, PHI exposure, or concentration risk - should move up to executive leadership or the board. Board reporting works best when it stays focused on critical vendors with open high-risk findings, overdue remediation items, and outage readiness for core services. Aligning the program to HIPAA Security Rule, NIST SP 800-161, and HITRUST CSF gives healthcare leaders a recognized structure for standardizing assessments, evidence requests, and remediation priorities across the supplier portfolio.[4][5]
Contingency Planning for Vendor Outages and Inherited Failures
Controls lower exposure. Recovery plans keep care moving when a vendor still goes down. After the Change Healthcare attack, 60% of nearly 1,000 affected hospitals needed two to three months to return to normal operations.[6]
Good contingency planning starts with a plain question: which vendor failures would stop clinical operations or the revenue cycle right away? From there, teams need manual workarounds for each case, and they need to test them on a regular basis. That can include:
- Paper-based pharmacy order workflows
- Offline patient registration
- Manual appointment management
- Backup claims submission paths
Recovery playbooks should spell out who does what, when they do it, and in what order. Those playbooks also need validation through tabletop exercises and live drills. If not, they often fall apart when several systems go down together or when one vendor outage ripples across dependent services. Keeping secondary vendors for high-concentration services, such as payment clearinghouses and diagnostic imaging storage, helps cut single points of failure.
At scale, all of this depends on a centralized view of supplier risk and response readiness.
Scaling Supply-Chain Risk Management With Censinet RiskOps™
These controls tend to break down when risk data is scattered across spreadsheets and email. Once a program sets vendor tiers and controls, it needs one workflow to put them into action.
How Censinet RiskOps™ centralizes third-party vendor risk management
Censinet RiskOps™ brings together assessments for suppliers, devices, and fourth-party relationships in one platform. Security teams get a single dashboard to track supplier, device, and fourth-party risk.
That shift to one workflow can pay off fast. Tower Health cut assessment cycle time from 5–6 weeks to under one week and tripled productivity.[10]
When all supplier data sits in one place, teams can automate the slowest parts of review instead of chasing updates across inboxes and files.
How Censinet AI™ Speeds Up Risk Decisions
Censinet AI™ helps teams move faster by summarizing questionnaires and evidence, flagging fourth-party exposure, and drafting risk summaries from assessment findings. Team review and approval stay built into the process, so risk teams keep control through configurable rules and review workflows.
Conclusion: Treat Supply-Chain Cyber Risk as a Patient Safety and Business Continuity Issue
Supply-chain attacks aren't a side issue anymore. 60% of healthcare data breaches in 2023 were caused by third-party vendors, costing organizations an average of about $10 million per incident.[11] And the damage doesn't stop at data exposure. It can disrupt patient care too. Doing all of this by hand just doesn't scale. Treat supply-chain cyber risk as a patient safety and business continuity issue.
FAQs
Why is healthcare supply-chain risk getting worse now?
Healthcare supply-chain risk is getting worse because the healthcare ecosystem is more digitally connected. That means a breach or disruption at just one vendor can ripple across many organizations.
The problem gets worse when providers rely on single-source suppliers, old legacy systems, and fragmented risk management. In many cases, teams still depend on static, manual assessments instead of continuous monitoring. Put that all together, and the fallout can hit operations, finances, and even patient safety.
Which vendors pose the biggest risk to hospitals?
The biggest risks usually come from vendors that act as a single point of failure in clinical or day-to-day operations. If that vendor goes down - and there aren’t many backup options - the damage can spread fast.
The highest-priority cases often include vendors tied to core clinical services, pharmacy automation, patient identity and consent systems, claims processing clearinghouses, and software used for medical device management and imaging.
So the goal isn’t to focus on vendor count alone. Hospitals need to rank vendors based on:
- Criticality: How much the workflow depends on them
- Fragility: How likely a disruption is, and how hard recovery would be
- Downstream impact: How far the problem would ripple across care delivery and operations
That gives a much clearer picture of risk than simply asking how many vendors are in the stack.
How can hospitals prepare for a vendor outage?
Hospitals need a patient-safety-first approach. Start by mapping each vendor to the clinical services it supports, then pinpoint critical dependencies and define acceptable downtime limits. From there, rehearse incident response and disaster recovery on a regular basis with procurement, IT, and clinical teams at the table.
It also helps to keep one central inventory of vendor services, data access, and security posture, backed by continuous monitoring. To cut risk, hospitals should:
- diversify suppliers
- segment device networks
- test offline backups
- include critical vendors in emergency protocols
