Re-identification risk in healthcare data is the chance that anonymized patient information can be traced back to individuals. Even after removing identifiers like names or Social Security numbers, attackers can use public records (e.g., voter lists) to link data points like birth dates, gender, and ZIP codes to real people. For instance, 63%-87% of the U.S. population can be identified using just these three details.
This risk matters because it can lead to privacy breaches, legal penalties, and loss of trust in healthcare systems. HIPAA offers two methods to reduce this risk: Safe Harbor, which removes specific identifiers, and Expert Determination, which uses statistical analysis to minimize risks while keeping data useful. However, no method guarantees complete anonymity.
Attackers often exploit "quasi-identifiers" through targeted (prosecutor model), event-driven (journalist model), or large-scale (marketer model) approaches. Organizations can mitigate risks by combining anonymization techniques like generalization or suppression with strict data-sharing controls, such as Data Use Agreements and secure access systems.
To manage these risks effectively, healthcare organizations should regularly measure re-identification probabilities using tools like ARX or Google Cloud Sensitive Data Protection. Combining technical safeguards with strong policies ensures data privacy without compromising its usefulness for research.
Healthcare Data Risks: HIPAA, PHI, and Re-identification #shorts
sbb-itb-535baee
HIPAA De-Identification Standards
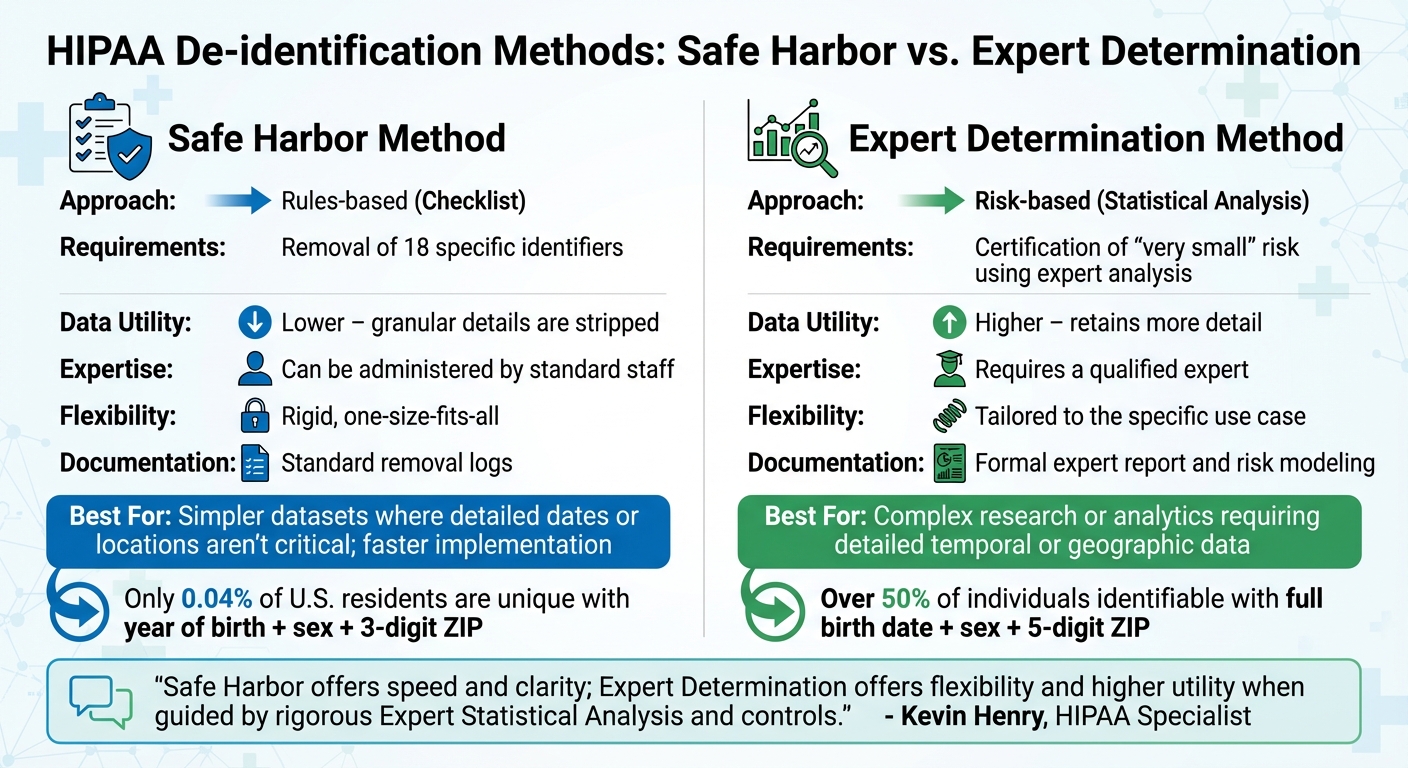
HIPAA Safe Harbor vs Expert Determination De-Identification Methods Comparison
HIPAA outlines two main methods for de-identifying health information: Safe Harbor and Expert Determination. Both are designed to minimize the risk of re-identifying individuals in datasets. The U.S. Department of Health and Human Services explains the goal clearly:
"Health information that does not identify an individual and with respect to which there is no reasonable basis to believe that the information can be used to identify an individual is not individually identifiable health information." [5]
Understanding these methods helps organizations decide which approach best fits their data needs and objectives.
Safe Harbor Method
The Safe Harbor method follows a straightforward checklist. It requires removing 18 specific identifiers, such as names, Social Security numbers, and medical record numbers. Additionally, certain dates and geographic details must be modified. For example, only the year can remain for dates, and ages over 89 must be grouped as "90 or older" [2]. ZIP codes are another critical element: only the first three digits can be kept if the area they represent includes more than 20,000 people. Otherwise, the ZIP code must be replaced with "000" [2].
While this method is simple and predictable, it can limit the dataset's usefulness. Research highlights how combinations of data can still pose risks. For instance, the combination of year of birth, sex, and a 3-digit ZIP code is unique for about 0.04% of U.S. residents, whereas combining full birth dates, sex, and 5-digit ZIP codes makes over 50% of individuals identifiable [2]. Organizations can assign unique codes to de-identified records for internal use, as long as these codes aren't derived from patient data and the mapping key is securely stored. Special attention is also required for free-text fields in clinical notes, as they might contain hidden identifiers that automated processes could miss [10].
While Safe Harbor is easier to implement, the Expert Determination method offers a more tailored approach, balancing privacy with data usefulness.
Expert Determination Method
Unlike Safe Harbor, the Expert Determination method uses a flexible, risk-focused approach. A qualified expert evaluates the dataset using statistical and scientific principles to ensure the risk of re-identification is "very small" [5] [9]. HIPAA requires these experts to have proven knowledge and experience in statistical methods [5], often from fields like statistics, mathematics, or related areas. Their expertise typically includes re-identification risk analysis and Statistical Disclosure Control [8] [11].
The expert works iteratively, assessing and adjusting the dataset until the risk is sufficiently reduced [2] [5]. There’s no fixed numerical threshold for what constitutes "very small" risk; the expert determines this based on the dataset, its intended audience, and its use case [2] [5].
Kevin Henry, a HIPAA Specialist at Accountable, explains the trade-off:
"Safe Harbor offers speed and clarity; Expert Determination offers flexibility and higher utility when guided by rigorous Expert Statistical Analysis and controls." [8]
This method allows organizations to retain more granular details - like specific dates or full ZIP codes - if the expert can demonstrate that the re-identification risk remains minimal [8]. The process must be documented thoroughly, with a formal report detailing the methods and findings [12]. Organizations should also set clear triggers for re-assessment, such as the release of new external datasets or changes in data scope. Pairing technical measures with safeguards like Data Use Agreements, which explicitly ban re-identification attempts, strengthens compliance [11] [8] [10].
| Feature | Safe Harbor Method | Expert Determination Method |
|---|---|---|
| Approach | Rules-based (Checklist) | Risk-based (Statistical Analysis) |
| Requirements | Removal of 18 specific identifiers [5] | Certification of "very small" risk using expert analysis [5] |
| Data Utility | Lower – granular details are stripped | Higher – retains more detail |
| Expertise | Can be administered by standard staff | Requires a qualified expert [7] |
| Flexibility | Rigid, one-size-fits-all | Tailored to the specific use case |
| Documentation | Standard removal logs | Formal expert report and risk modeling [12] |
The Safe Harbor method is ideal for simpler datasets where detailed dates or locations aren’t critical. It’s faster and easier to implement for regulatory purposes [9]. On the other hand, Expert Determination is better suited for more complex research or analytics that require detailed temporal or geographic data, such as population health studies. Implementing these standards is part of a broader strategy for healthcare risk operations to ensure patient safety and data integrity. For HIPAA compliance, documentation should typically be retained for six years [10].
Both methods play a crucial role in managing re-identification risks, helping organizations responsibly handle healthcare data while meeting regulatory standards.
Common Re-Identification Scenarios and Attack Models
Even with HIPAA de-identification measures in place, attackers can still piece together datasets to uncover individuals' identities by analyzing patterns in the data. Understanding these methods is vital for organizations aiming to spot and address weak points before they are exploited. There are three primary attack models - prosecutor, journalist, and marketer - which rely on linking common "quasi-identifiers" like age, gender, and ZIP code with external information. These models highlight the risks associated with re-identification and the various strategies attackers employ.
Prosecutor, Journalist, and Marketer Attack Models
The prosecutor model involves a highly targeted approach. Here, the attacker focuses on a specific person, knowing their record exists within the dataset [3][1]. These attackers often have detailed background knowledge - perhaps as a researcher, expert witness, or someone familiar with the individual - and aim to confirm a match by cross-referencing overlapping details.
The journalist model also targets a specific person but without certainty that the individual’s data is in the dataset [14]. This method often exploits "newsworthy" events, such as celebrity illnesses or major accidents, to connect public incidents with de-identified records [14][4]. A well-known example occurred in 2006, when a journalist from The New York Times identified a user from a supposedly "anonymized" AOL dataset. By analyzing search queries containing geographic locations and surnames, the journalist identified Thelma Arnold, a 62-year-old widow from Lilburn, Georgia [4].
The marketer model takes a broader approach, aiming to re-identify as many individuals as possible rather than focusing on a single target [1]. This large-scale tactic often involves linking entire datasets, such as combining medical records with voter registration lists, to create detailed profiles for commercial purposes. As researchers Kathleen Benitez and Bradley Malin explain:
"Anytime there is a level of individuality, or distinctiveness, there is the potential for re-identification" [14][1].
These models exploit residual quasi-identifiers in de-identified data. Research shows that 87.1% of the U.S. population can be uniquely identified using just a 5-digit ZIP code, birth date, and gender. When more specific attributes are included, re-identification rates can soar to 99.98% [14][15].
Sources of Linkage Vulnerabilities
Attackers rely on external data sources to enhance their re-identification efforts. Surprisingly, sophisticated tools aren't always necessary - access to the right external datasets often suffices.
Voter registration lists are a particularly potent resource. These lists typically include names, addresses, ZIP codes, dates of birth, and gender for large portions of the population, and their cost varies by state [4][1].
News media and public reports also play a significant role, especially for individuals involved in high-profile incidents like motor vehicle accidents. For example, researchers from the State University of New York at Buffalo conducted a re-identification study on a database of 242,343 patients. Focusing on 14 "high-risk" patients involved in serious accidents, they successfully re-identified 4 individuals - 28.6% of the targeted group - by linking accident details to online news archives [14]. In one case, a victim’s name was found in the comments section of a news article, even though the article itself withheld the name [14].
Other sources, such as social media profiles, vital records (e.g., birth, death, and marriage registries), and consumer databases (containing purchase history or credit information), further aid attackers [3][5]. Researchers Arvind Narayanan and Vitaly Shmatikov emphasize:
"Linkability of data, not the sensitivity of data, is the key to re-identification risk" [14].
Even seemingly minor details, like a note documenting a motor vehicle accident, can dramatically increase re-identification risks. For instance, such documentation raises the risk by 537 times compared to the general population. For patients hospitalized with permanent injuries from an accident, the re-identification risk can climb as high as 66.67% [14].
Recognizing these vulnerabilities is essential for developing effective defenses, which can be informed by healthcare cybersecurity benchmarks and will be explored in later sections.
| Attack Model | Primary Goal | Knowledge Level | Typical Linkage Source |
|---|---|---|---|
| Prosecutor | Identify a specific individual known to be in the data | High (full knowledge of target) | Private records, banking data, or direct knowledge [3][1] |
| Journalist | Identify a specific individual from a public event | Medium (partial data) | Newspaper archives, social media, public news sites [14] |
| Marketer | Identify the maximum number of records possible | Variable (large-scale) | Voter registration lists, public census data, consumer databases [1] |
Assessing and Measuring Re-Identification Risk
Understanding re-identification scenarios is just the beginning. To truly grasp the risk, it’s essential to measure both the likelihood and impact of an attack. The HHS Office for Civil Rights puts it succinctly:
"Risk can be understood as a function of 1) the likelihood of a given threat triggering or exploiting a particular vulnerability, and 2) the resulting impact on the organization" [20].
This boils down to two key factors: Severity (how damaging it would be if someone's identity were exposed) and Likelihood (how probable it is that an attack could succeed). Severity depends on the sensitivity of the information - exposing a cancer diagnosis is far more serious than revealing a flu vaccination. Likelihood, on the other hand, is influenced by Exposure, which measures how easily quasi-identifiers in the dataset can be linked to external information, and whether sensitive details can be inferred from them [16].
To evaluate these risks systematically, a combination of frameworks and testing methods can be applied.
Risk Assessment Frameworks
Statistical frameworks are commonly used to measure re-identification risks by examining how unique individuals appear in a dataset. Here’s a breakdown of some key approaches:
- K-anonymity: Ensures each individual is indistinguishable from at least k-1 others based on quasi-identifiers like age, gender, or ZIP code [18][19]. However, even in a k-anonymous group, sensitive information can still be exposed if all members share the same condition.
- L-diversity: Improves on k-anonymity by requiring diversity in sensitive attributes within each group, preventing "homogeneity attacks" where everyone in the group has identical conditions [18][19].
- T-closeness: Adds another layer of protection by ensuring that the distribution of sensitive attributes within a group closely matches the distribution across the entire dataset [13].
- δ-presence: Useful for datasets where mere membership is sensitive (e.g., a cancer registry). This method estimates the probability that a specific individual is included in the dataset [18][19].
When using these frameworks, it’s critical to include entity identifiers to account for individuals who appear in multiple records. Ignoring these identifiers could lead to inflated k-anonymity values, giving a false sense of security [19].
Direct Testing with External Datasets
Statistical models are valuable, but testing your dataset against external sources provides a more practical risk estimate. One effective method is simulating an attack to see how easily quasi-identifiers in your data could be matched with public records like voter lists, census data, or mortality databases [3].
For example, the Mental Health Research Network (MHRN) tested a dataset of 20 million visits by checking for overlaps with state mortality records. They found that combining Hispanic ethnicity, female gender, age 13–17, and a 2012 overdose death in Washington state reduced the pool to just three individuals - matching 15 records in the state’s identifiable mortality database [3].
This approach requires assessing the population overlap between your dataset and external sources. Risk is highest when the populations are congruent (completely overlapping), lower when your dataset is a random subset, and lowest with partial overlap. As Gregory E. Simon, MD, MPH, from Kaiser Permanente explains:
"The uniqueness of any record depends not on the distribution or frequency of any single variable but rather on the potential cross-classification of multiple variables" [3].
Direct testing also factors in economic barriers, with re-identification costs ranging from $0 to $17,000 per record [1].
Comparison of Risk Models
Different attacker models require tailored approaches to calculate probabilities and mitigate risks. The table below outlines how these models operate:
| Attack Model | Attacker Knowledge | Probability Calculation | Primary Mitigation Strategy |
|---|---|---|---|
| Prosecutor | Knows the target is in the dataset [16][17] | Inverse of the equivalence class size within the dataset [16][17] | Increase k-anonymity to create larger equivalence classes [19] |
| Journalist | Unsure if the target is in the dataset; relies on population uniqueness [16][17] | Probability that a subject is unique in the overall population (k-map) [16][17] | Compare dataset against larger populations like the US Census [19] |
| Marketer | Aims to re-identify as many individuals as possible [16][17] | Average re-identification probability across the dataset [16][17] | Reduce uniqueness through generalization and suppression [1] |
For unknown population sizes, models like Pitman can provide accurate estimates of uniqueness [17].
Quantifying risk accurately is the foundation for the mitigation strategies discussed next.
Mitigating Re-Identification Risks
Once risks have been measured, the next step is to reduce them to a "very small" level while maintaining the data's usefulness. This often involves anonymizing the data and controlling how it is accessed. As Mehmet Kayaalp, MD, PhD, from the U.S. National Library of Medicine, explains:
"The de-identification process minimizes the risk of re-identification but has no claim to make it impossible" [22].
The best approach depends on factors like the intended users, the purpose of the data, and its sensitivity. Building on earlier risk assessment methods, organizations can develop customized de-identification strategies that strike a balance between privacy and usability. Below are specific techniques and controls that can help achieve this balance.
Data Anonymization Techniques
Generalization reduces the specificity of data, making it harder to identify individuals. For instance, instead of including a full date of birth, you might only include the year, or you could shorten a five-digit ZIP code to just the first three digits. This shift significantly lowers the chances of identifying someone. A full date of birth, sex, and five-digit ZIP code can uniquely identify over 50% of U.S. residents, but switching to a year of birth and a three-digit ZIP code drops that uniqueness to just 0.04% [2].
Suppression involves removing specific data fields that could make someone easily identifiable [22]. Pseudonymization replaces direct identifiers, such as "James Smith", with generic tags like "John Doe" or placeholders like "[Personal Name]" [22]. Perturbation subtly alters data values, making it harder to link records to external datasets [2]. Differential privacy takes a different approach by adding statistical noise to query results. The U.S. Census Bureau uses this method to ensure that even repeated queries cannot reveal whether a particular individual is in the dataset [23].
Automated tools, like NLM-Scrubber, can efficiently process clinical reports to remove identifiers, but manual review is still necessary to catch nuanced, context-specific identifiers [22].
A risk-based de-identification strategy is often the most effective. Experts tailor techniques to the dataset and its audience, ensuring both privacy and utility. As Privacy Analytics explains:
"By measuring the risk, organizations can apply a risk-based de-identification strategy that simultaneously protects the individual but also enables the secure release of granular data" [21].
This approach might include creating multiple versions of a dataset. For example, one version could include detailed geographic data but generalized age information, while another might provide precise ages but less specific location data. Experts should also set time limits on certifications, as new technologies and external data sources can change risk levels over time [2].
Controlled Data Sharing Mechanisms
Even after de-identifying data, controlled sharing mechanisms are critical to further reduce exposure. These include both legal and technical measures. Data Use Agreements (DUAs) are a key legal tool that restrict access to data and explicitly prohibit re-identification [3][25]. DUAs can also prevent recipients from combining datasets in ways that might inadvertently reveal identities [5]. Under HIPAA, researchers using Limited Data Sets - which may retain certain identifiers like dates or town-level geography - must sign a DUA [22].
Hierarchical access rating is another safeguard that matches the level of data detail to the trustworthiness of the recipient. Dingyi Xiang from the Internet Rule of Law Institute highlights this concept:
"The level of trust for a data recipient becomes a critical factor in determining what data may be seen by that person" [24].
For example, low-trust users might only access aggregated data with added noise, while highly vetted researchers working within secure systems could access more detailed information. Secure data enclaves offer another layer of protection by keeping raw data on a central server. Users can run queries through a controlled interface without ever downloading the actual records [3]. Network isolation ensures that only de-identified or encrypted data is transferred between clinical and research environments using firewalls and proxy servers [24]. Meanwhile, federated learning allows institutions to share machine learning model parameters rather than raw patient data, keeping sensitive information on-site [24].
Organizations should also follow the minimum necessary principle, sharing only the smallest amount of identifiable information required for legitimate research or public health purposes [25]. To further bolster security, staff with access to identifiable data should complete annual training and re-sign confidentiality agreements. A designated Overall Responsible Party (ORP) should oversee data security and handle any potential breaches [25].
Tools for Evaluating and Managing Re-Identification Risk
Healthcare organizations need reliable tools to assess and manage the risk of re-identification. These tools help identify vulnerable quasi-identifiers, calculate risk scores, and ensure compliance with HIPAA standards. As the U.S. Department of Health and Human Services (HHS) puts it:
"Risk analysis is the first step in an organization's Security Rule compliance efforts... it should provide the organization with a detailed understanding of the risks to the confidentiality, integrity, and availability of e-PHI." [20]
Here’s a look at some of the tools that support risk evaluation and management.
Statistical Disclosure Control Tools
The ARX Data Anonymization Tool is an open-source solution designed to apply privacy models like k-anonymity, l-diversity, t-closeness, and differential privacy to healthcare data. It evaluates risk under three attacker scenarios: the prosecutor model (where the attacker knows the individual is in the dataset), the journalist model (where membership is uncertain), and the marketer model (who targets as many individuals as possible) [17] [16].
Google Cloud Sensitive Data Protection (formerly Cloud DLP) is another powerful tool. It calculates re-identification metrics such as k-anonymity, l-diversity, k-map, and δ-presence for structured data in BigQuery [18] [19]. When using k-anonymity, it’s important to incorporate entity IDs to account for patients appearing in multiple rows [19].
For smaller practices, the HIPAA Security Risk Assessment (SRA) Tool, developed by the ONC and OCR, helps identify vulnerabilities and align with HIPAA Security Rule requirements [20].
These statistical tools are just the beginning - integrated platforms take risk management further.
Censinet RiskOps™ for Risk Management
Censinet RiskOps™ provides a centralized platform for automating risk assessments and identifying linkage vulnerabilities that could lead to re-identification. This platform simplifies workflows, making it easier for healthcare organizations to manage risks tied to patient data and PHI.
Adding to its capabilities, Censinet AI™ speeds up the risk assessment process by summarizing vendor evidence, capturing product integration details, and generating risk summary reports. It uses a blend of automation and human oversight to validate evidence and mitigate risks. The platform also features real-time dashboards that direct critical findings to the right stakeholders, acting as a command center for risk management.
Comparison of De-Identification Techniques
Choosing the right de-identification method can make a big difference in managing re-identification risks. Here's a quick comparison:
| Method | Difficulty | Effectiveness | Data Utility |
|---|---|---|---|
| Safe Harbor | Low; focuses on removing key identifiers [13] [3]. | Moderate; may leave privacy gaps [16] [13]. | Low; often limits data usability [16] [13]. |
| Expert Determination | High; requires evaluation by statistical experts [13] [3]. | High; uses tailored, risk-based frameworks [13]. | High; balances data utility and low risk [3]. |
Organizations should pay close attention to attributes like demographics and ZIP codes, as these are often easily accessible in auxiliary datasets and can be used in linkage attacks [16]. Risk analysis isn’t a one-and-done process - it should be revisited whenever new technologies, ownership changes, or additional data sources come into play [20] [13].
The growing importance of these tools is reflected in the data masking market, which is expected to expand from $1.08 billion in 2025 to $2.14 billion by 2030 [16].
Conclusion
Re-identification risk isn't just a compliance box to check - it’s a genuine threat that can impact patient privacy, organizational trust, and legal compliance. As discussed earlier, even harmless-looking data points can combine to uniquely identify a large percentage of individuals [1][13]. The consequences are severe: re-identification can result in patient harm, discriminatory practices, and financial penalties that can reach millions of dollars.
To address this, a multi-layered approach is essential. This means leveraging HIPAA’s de-identification methods alongside technical tools like k-anonymity and l-diversity, while also implementing administrative measures such as Data Use Agreements that explicitly prohibit re-identification attempts. Kevin Henry, a recognized HIPAA authority, emphasizes:
"Re-identification risk is manageable when you combine sound de-identification, rigorous Risk Assessment, disciplined governance, and modern tooling" [6].
The evolving landscape of AI and the growing availability of public datasets make regular reassessment critical - ideally every year or whenever there are changes to datasets [6]. Platforms like Censinet RiskOps™ are instrumental in this process, automating risk assessments, streamlining communication of findings, and offering real-time dashboards to monitor vulnerabilities. These tools are central to staying ahead of re-identification threats in today’s data-driven healthcare environment.
Striking the right balance between data utility and privacy is essential for fostering both innovation and trust. Organizations that prioritize privacy not only avoid penalties but also earn patient confidence, positioning themselves as leaders in safeguarding sensitive health information. By following the strategies and tools outlined here, healthcare organizations can responsibly unlock the potential of their data while protecting the individuals they serve.
FAQs
When should we use Safe Harbor vs Expert Determination?
For a straightforward and budget-friendly method to de-identify healthcare data, consider using Safe Harbor. This approach involves removing 18 specific identifiers from the data, making it a practical choice for achieving HIPAA compliance in cases like low-risk data sharing or basic research projects.
On the other hand, if your work demands detailed datasets for advanced analytics or AI applications, Expert Determination is the better option. This method relies on a qualified expert to evaluate the risk of re-identification. While it offers greater data utility, it does require more effort and specialized expertise to implement effectively.
What quasi-identifiers create the highest re-identification risk?
Quasi-identifiers that pose the greatest risk for re-identification might surprise you. They often include data that seems harmless at first glance, such as geographic areas smaller than a state, specific dates (excluding the year), ages over 89, and unique details like ZIP codes. When combined, these pieces of information can create a unique profile, making it possible to identify individuals. This is why managing these elements carefully is so important, especially in the context of healthcare data.
How often should we reassess re-identification risk?
Revisiting re-identification risks is not a one-and-done task - it’s something that should happen regularly, especially when changes occur in the healthcare data landscape. Experts often suggest performing these assessments annually, but they should also happen whenever there are updates to systems, data handling procedures, or security measures.
Events like adopting new data collection methods, implementing policy changes, or introducing new technologies can bring about fresh risks. Addressing these promptly helps ensure compliance with regulations such as HIPAA and keeps sensitive information protected.
