Healthcare AI now carries direct compliance, patient-safety, and contract risk. If I were leading AI oversight in a U.S. health system today, I’d focus on seven things first: protect PHI, approve use cases before launch, test models in local care settings, check vendor chains, watch for bias, prepare for AI incidents, and tie all of it to enterprise risk.
Here’s the short version:
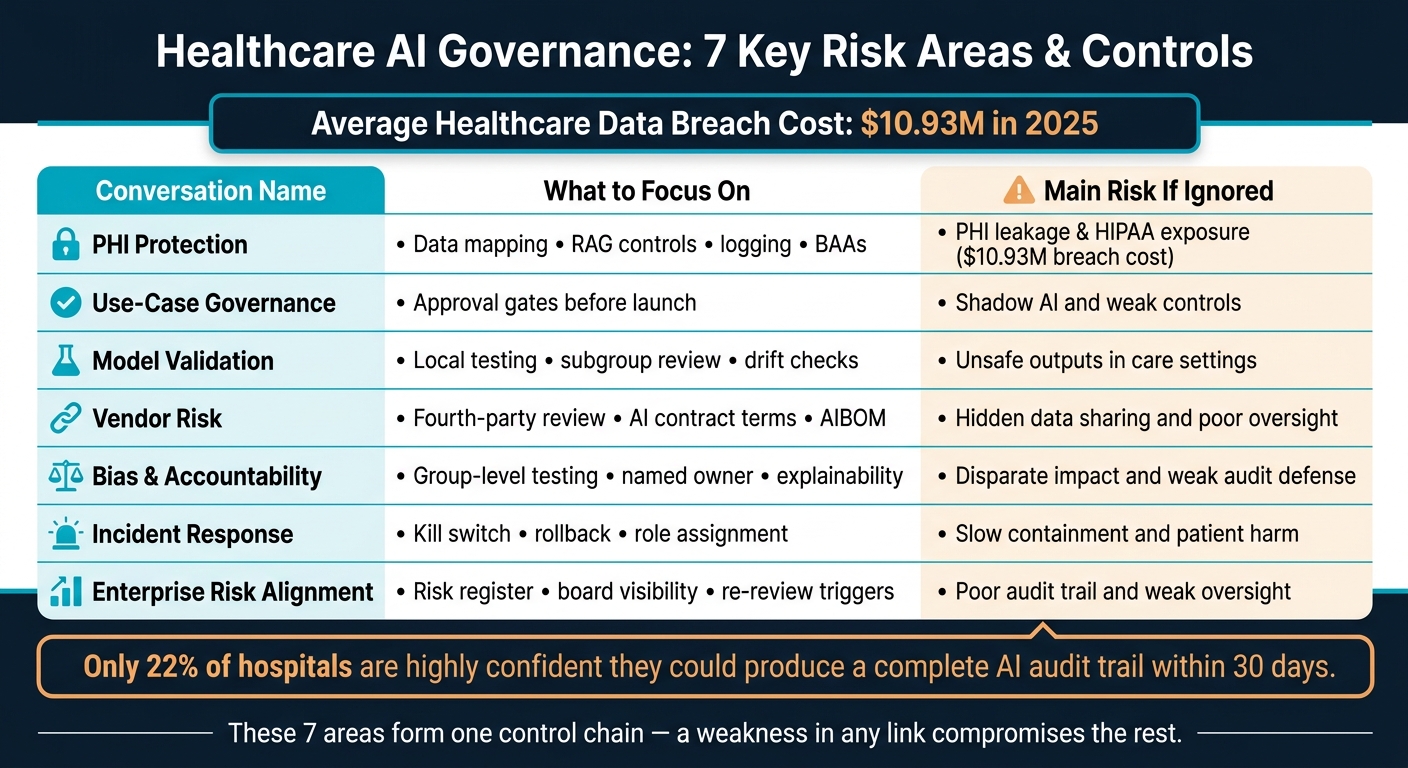
- PHI exposure is the first problem to fix. The article points out that healthcare breach costs hit $10.93 million in 2025, and AI expands where PHI can enter, move, and stay.
- Governance has to happen before deployment. That means checking BAA coverage, data location, logging, user access, and use-case risk before any tool goes live.
- Local validation still matters. FDA clearance does not mean a model is safe for your patients, your staff, or your workflow.
- Vendor review has to go deeper. It’s not just the main vendor. It’s subprocessors, model hosts, cloud providers, and any hidden AI features added later.
- Bias and explainability are not side issues. If a model treats groups differently or no one can explain an output, audit and care risk both go up.
- AI incidents need their own playbooks. Unsafe outputs, PHI leakage, prompt injection, model drift, and vendor compromise need clear shutdown and rollback steps.
- Board and risk teams need proof, not slides. Model inventory, logs, owners, version history, and re-review triggers should all connect back to the risk register.
Healthcare AI Governance: 7 Key Risk Areas & Controls
From Deployment to Oversight: Strengthening AI Risk Management and Patient Safety in Health Care
sbb-itb-535baee
Quick Comparison
| Conversation | What I’d focus on | Main risk if ignored |
|---|---|---|
| PHI protection | Data mapping, RAG controls, logging, BAAs | PHI leakage and HIPAA exposure |
| Use-case governance | Approval gates before launch | Shadow AI and weak controls |
| Model validation | Local testing, subgroup review, drift checks | Unsafe outputs in care settings |
| Third-party risk | Fourth-party review, AI contract terms, AIBOM | Hidden data sharing and poor oversight |
| Bias and accountability | Group-level testing, named owner, explainability | Disparate impact and weak audit defense |
| Incident response | Kill switch, rollback, role assignment | Slow containment and patient harm |
| Enterprise risk alignment | Risk register, board visibility, re-review triggers | Poor audit trail and weak oversight |
My takeaway is simple: this isn’t a list of separate tasks. It’s one control chain. If one link is weak, the rest are harder to trust.
Below, I’d treat each conversation as a standing risk item, not a one-time project.
1. Safeguarding PHI Across AI Workflows
PHI now moves through a lot more than one system. So the first step is simple: map where PHI enters, where it moves, and where it stays.
In AI workflows, PHI can come in through prompts, AI scribes, voice agents, and EHR integrations. From there, it can move through cloud transfer, model inference, and RAG pipelines, where it may be converted into embeddings and stored in vector databases. That means you can't treat these workflows like plain software. The data path is longer, messier, and riskier.
Embeddings created from PHI are derived PHI under 2025 OCR guidance. That makes RAG design a compliance matter, not just an engineering call.[1]
Use the right controls at each stage:
| Workflow Stage | PHI Activity | Required Controls |
|---|---|---|
| Entry | Prompts, voice/audio, EHR data | Consent workflows, MFA, Role-Based Access Control (RBAC) |
| Processing | Inference, RAG, embeddings | Enclave-based processing, tokenization |
| Movement | Cloud transfer, subprocessors | BAAs with all downstream processors and contractually required U.S.-based residency |
| Exit/Storage | Logs, model weights, summaries | Immutable audit logs, SIEM integration |
Contracts need close attention too. A plain BAA doesn't do enough here. The agreement should clearly ban model training on PHI, name every downstream subprocessor, and require a technical training-data opt-out instead of leaning on a vendor policy statement.[1]
The 2024 Montefiore Medical Center settlement of $4.75 million showed what weak audit controls and poor access-log monitoring can cost.[1] With AI, the standard gets higher. Logs need to show who accessed the data and what the system returned. HIPAA also requires six-year retention under 45 CFR 164.530(j).[1]
Once PHI is under control, leaders need to decide which AI use cases can go live.
2. Governing AI Use Cases Before Deployment
Every healthcare AI use case needs a governance review before deployment. That step helps cut compliance, safety, and audit risk before anything reaches production. It’s the point where cybersecurity, privacy, and clinical safety have to line up.
The review should cover four pillars: BAA chain coverage, data residency, authoritative audit trail, and risk tiering by clinical impact, PHI exposure, and downstream decisions. Workforce controls also need to sit inside the approval gate.
Here’s how the core pre-deployment requirements map out:
| Governance Pillar | Pre-Deployment Requirement |
|---|---|
| BAA Chain | Confirm every external service touching PHI remains within an active BAA and approved workload scope. |
| Data Residency | Keep high-risk PHI workloads on-prem or in a hospital-controlled VPC; route lower-risk use cases only through BAA-covered external services. |
| Authoritative Audit Trail | Log prompts, outputs, user identity, and timestamps to the hospital SIEM before launch. |
| Risk Tiering by Clinical Impact | Tier the use case by clinical impact, PHI exposure, and downstream decisions; validate for accuracy, bias, calibration, and edge-case behavior before launch. |
| Workforce | Verify SSO-bound identities and require browser-level DLP and attestation. |
Put simply, governance decides what can launch; validation decides whether it should.
Governance also needs to stop shadow AI, not just react to it. The best way to do that is to steer staff toward approved tools backed by enforced controls [3].
Approval shouldn’t sit with one team alone. A cross-functional committee - including the HIPAA privacy officer, security, clinical informatics, legal, and the relevant operational leader from the impacted service line - should approve each use case [3].
Once a use case clears governance, leaders still need to prove it performs safely in clinical conditions.
3. Validating Model Performance and Clinical Safety
A lot of healthcare organizations dodge the hard part: checking whether a model works safely with their patients, their staff, and their data. For healthcare leaders, validation isn't a box to check. It's a patient-safety guardrail and a risk-control step. Once a use case gets approved, the next issue is simple: does it work safely in actual clinical conditions?
The stakes are high. A diagnostic AI that misses sepsis or slows down a stroke diagnosis can hurt patients. A coding model that invents clinical details can damage the medical record and create billing fraud exposure. One cross-sectional analysis of 950 FDA-authorized AI medical devices found 182 recall events across 60 devices, with higher recalls among devices that lacked clinical validation. More than 43% of those recalls happened within 12 months.[5][8] That timing matters because recalls tend to bunch up early.
FDA authorization doesn't remove the need for local testing. FDA 510(k) clearance does not prove that a tool will perform well in your patient population or fit your workflow. Health systems still need context-specific validation, even for cleared tools.[5][9]
High-risk use cases need the most scrutiny. That includes diagnostic support, predictive deterioration models, and treatment recommendations. These tools should go through prospective evaluation, independent clinical review, and human confirmation before their outputs shape decisions. Lower-risk use cases, like ambient documentation or patient education, still need guardrails too. Set error thresholds. Build clear escalation paths.
Across every risk tier, subgroup analysis is non-negotiable. Performance should be broken out by race, age, sex, and disease severity so teams can spot disparities before deployment, not after.[4][5][10]
Validation also doesn't stop at go-live. Teams should keep watching for drift, hallucination rates, and data quality issues, with threshold-based alerts in place. And the response shouldn't be improvised. Decide ahead of time what happens next:
- heightened review
- restricted use
- retraining
- rollback
Staff training matters just as much. Programs should directly address automation bias and cognitive anchoring. If the interface makes the model sound certain all the time, people may trust it too much. That's why the UI should show uncertainty, confidence scores, and known limits instead of presenting outputs as if they were final answers.[5][6][7]
| Validation Layer | What to Assess | High-Risk Requirement |
|---|---|---|
| Technical | Accuracy, precision, recall, calibration, robustness | Prospective testing on a representative cohort |
| Clinical | Clinician benchmark performance, subgroup equity | Independent clinical review committee sign-off |
| Workflow | Usability, human factors, integration behavior | Human confirmation before outputs drive decisions |
| Ongoing | Data drift, hallucination frequency, incident signals | Continuous monitoring with threshold-triggered alerts |
Even when performance looks good at launch, vendor controls still matter. Third-party AI services can add new risk after deployment.
4. Managing Third-Party and Fourth-Party AI Risk
Even tools that pass review can open the door to new risk the moment data leaves your environment. Approving a vendor's AI tool is just the start. In many cases, the bigger problem sits deeper in the stack: subcontractors, foundation model providers, and cloud hosts. That's where many healthcare groups lose the thread. Once data moves into a vendor's AI pipeline, it can become hard to tell who is touching it and where it goes next.
The core problem is visibility. Once PHI enters an AI vendor pipeline, health systems often lose sight of subcontractors, model hosts, and cloud layers.
Standard BAAs don't deal with AI supply-chain risk. AI contracts need to spell out the full data path. Vendors should list every downstream subprocessor in the BAA itself, and the contract should ban any training or fine-tuning on PHI. It should also confirm that sub-BAAs cover every fourth party touching PHI. If a vendor can't show that sub-BAAs cover each fourth party handling PHI, stop the review. Add a right to audit, along with a termination clause that covers destruction of derived data and model weights.[1]
One tool getting more attention is the AI bill of materials, or AIBOM. It maps model dependencies, open-source components, APIs, and downstream providers.[11][12] Also watch for silent AI - new AI features slipped into routine product updates without a new procurement review. A long-term vendor shouldn't get a free pass just because they've been around for years. If they add AI features, they need the same review as a new vendor.[11]
| Due Diligence Domain | Traditional Requirement | AI-Specific Requirement |
|---|---|---|
| Data Usage | Storage and access limits | Prohibit training or fine-tuning on PHI [1] |
| Transparency | Software versioning | AI bill of materials and vendor supply-chain map [11] |
| Security | Encryption at rest and in transit | Protected inference processing [1] |
| Monitoring | Uptime and availability | Drift, bias, and output accuracy [11] |
| Termination | Data return and deletion | Destruction of derived data and model weights [1] |
Vendor controls matter, but they don't fix bias, opacity, or murky accountability in model outputs.
5. Addressing Bias, Opacity, and Accountability Gaps in AI
Once vendor risk is covered, attention shifts to model behavior. The next issue is simple: does the AI treat patients fairly, and can the organization explain what happened when it doesn't?
Bias in healthcare AI is both a patient-safety issue and a compliance risk. A 2019 study found that a widely used hospital risk algorithm understated Black patients' care needs because it used spending as a stand-in for illness burden.[20] OCR's 2024 nondiscrimination rule now says covered entities must take reasonable steps to spot and reduce discriminatory effects in AI-enabled care.[14][16]
That problem gets worse when a model can't explain its output. Opacity makes bias harder to spot and harder to defend. If clinicians can't tell why a model flagged a patient, they can't make a sound call on whether to trust it, question it, or override it. Auditors run into the same wall. They lose a clear basis for explaining adverse decisions.[15]
Before go-live, review whether the training data matches the patient population across race, ethnicity, age, language, insurance status, geography, and major comorbidities. Then require subgroup testing against preset fairness thresholds for:
- False negatives
- False positives
- Calibration
- Sensitivity
Those thresholds should be a launch condition, not a nice-to-have.[14][4] ONC's HTI-1 transparency framework fits this approach because it requires disclosure of development, validation, and known limits.[17][18]
After deployment, keep watching subgroup outcomes as a standing control. If disparity signals show up, pause use and revalidate.[13][14]
Accountability is where many organizations stumble. Every AI use case needs one named owner for approval, monitoring, escalation, and retirement. Clinicians still own individual care decisions, and AI outputs stay advisory. Compliance and risk teams own regulatory alignment, while executive sponsors own program oversight and board reporting.[17][19]
When ownership is fuzzy, AI bias turns into risk that nobody fully owns. That weakens board reporting, slows incident escalation, and makes audit defense harder. If bias, drift, or opacity lead to harm, the incident response process should already spell out who owns the issue, how it gets escalated, and what containment looks like.
6. Preparing for AI-Driven Incidents
Once accountability is clear, leaders need to answer a tougher question: How do we spot and contain AI failure?
That’s where things get tricky. AI incidents usually don’t look like standard cybersecurity events. They show up as unsafe recommendations, skewed prioritization, or incorrect discharge text. In plain terms, this is not just a security issue. It’s a clinical and operational monitoring issue too.
That means detection can’t rely on firewall alerts alone. It needs a mix of:
- performance monitoring
- clinician feedback
- fairness checks
You should plan for five AI incident types: unsafe recommendations, PHI leakage, adversarial manipulation, scale errors, and vendor compromise.
AI incident response also needs three controls that standard playbooks often miss: kill switches, rollback to the last validated version or manual workflow, and redeployment criteria that require revalidation, bias testing, and approval. These are the day-to-day response tools for failed validation and monitoring. If a model drifts or starts producing unsafe outputs, these controls help stop the damage before it spreads.
After roles are assigned, the next step is to connect incident response to regulatory reporting and enterprise escalation. AI/ML device recalls often come from algorithm errors, drift, or workflow mismatch. FDA draft guidance for AI-enabled devices puts weight on postmarket monitoring and correction plans, which means incident response brings documentation duties and compliance exposure with it.[1][2]
An AI incident can trigger patient-safety risk, PHI risk, and compliance risk all at once. So ownership has to be clear before anything goes wrong.
- The CISO owns technical containment.
- The CMIO owns clinical risk assessment and provider communication.
- Compliance owns regulatory reporting and documentation.
These roles should be assigned in advance and practiced inside a broader AI oversight structure that also includes the CIO, privacy, and risk management. AI-specific tabletop exercises can help here, especially for biased triage and vendor-side breach scenarios. Those drills make it easier to define when an event stops being an IT incident and turns into a compliance issue or a board-level risk.
7. Connecting AI Oversight to Compliance and Enterprise Risk
AI governance needs a direct link to compliance and enterprise risk. If it doesn’t, gaps show up fast. The point is simple: turn AI oversight into a control layer that compliance, security, and risk teams can audit without guesswork.
In healthcare, AI oversight now reaches across FDA, HIPAA/HITECH, CMS, FTC, FCC, and state disclosure rules. That means compliance is no longer just a legal box to check. It can affect reimbursement, and state rules add yet another layer to manage. The table below shows where each regulator applies pressure and what part of AI use they care about most. [21][22]
| Agency | Regulatory Focus | Key Compliance Surface |
|---|---|---|
| FDA | Medical Devices / SaMD | Clinical Decision Support (CDS) classification; Predetermined Change Control Plans |
| OCR (HHS) | HIPAA & Privacy | BAAs, AI training data flows, technical safeguards |
| FTC | Consumer Protection | Marketing claims, "AI washing", terms of service |
| CMS | Reimbursement & Innovation | TEMPO and ACCESS models; tying compliance to revenue |
| FCC | Communications (TCPA) | Consent and disclosure for AI-generated calls/texts |
Of course, these duties don’t mean much on their own. They need to be tied to an AI risk register, named owners, and clear re-review triggers. Otherwise, rules sit on paper while models keep moving in production.
On the enterprise risk side, board oversight has to go beyond slide decks. Leaders need direct access to the model registry, access controls, logging, and incident response records. [23] If the board can’t see how models are tracked, changed, and shut down, oversight is thin when it matters most.
That’s why an AI risk register matters so much. It should track each use case, its approved data sources, and its rollback plan. It also needs mandatory re-review after version changes, data-source changes, or metric drift. [23] Without that, one model update can quietly change the risk picture overnight.
The current gap is hard to ignore. Only 22% of hospitals are highly confident they could produce a complete AI audit trail within 30 days for regulators. [24] That number says a lot. Many groups are using AI, but far fewer are set up to prove what happened, who approved it, what data fed it, and how it was monitored.
One practical way to put this into day-to-day work is to map AI oversight to the NIST AI RMF functions: Govern, Map, Measure, and Manage. The NIST AI Risk Management Framework gives teams a usable structure for lining up AI oversight with HIPAA administrative safeguards. When program pieces like AI asset inventory, BAA confirmation, algorithm monitoring, and incident response are mapped to specific HIPAA anchors, compliance teams get one auditable control set they can actually use. [22]
Vendor AI Risk Review Snapshot
Once third-party vendor risk management is done, the next step is contract control. This is where things get very concrete: the vendor agreement spells out how AI can handle PHI outside your environment. In plain English, contracts often determine whether a healthcare AI deal is defensible or left exposed.
The average healthcare data breach hit $10.93 million in 2025, up from $9.77 million in 2024.[1] That turns vendor review into a money issue, not just a compliance box to check. This requires a strategic approach to effectively manage third-party risk across the enterprise.
At a minimum, require:
- AI-specific BAAs
- Full subprocessor and foundation-model disclosure
- Advance notice for model changes
- Clear bans on PHI training
- Immutable log access
The table below shows the procurement checks that matter most, with a focus on three outcomes: PHI exposure, model change control, and auditability.
| Review Dimension | Acceptable Practice | High-Risk Practice |
|---|---|---|
| PHI/PII Handling | De-identification via Expert Determination; encryption during inference via confidential computing | Decryption in memory with no protections; Safe Harbor only |
| Model Training | Contractual opt-out or explicit opt-in for any use of customer PHI; technical blocks preventing ingestion | "Right to use data for product improvement" buried in standard ToS |
| Incident Notification | 72-hour notification | 60-day HIPAA maximum |
| Certification | HITRUST r2 Validated assessment; SOC 2 Type II | Self-assessments only; no independent third-party audit |
One point deserves extra attention: PHI-generated embeddings in RAG and vector databases should be treated as PHI during contract review, before signature.[1]
And that’s only part of the picture. These contract terms matter, but they don’t do much on their own if the organization isn’t also watching model behavior, log access, and data use after go-live.
AI Validation and Monitoring Requirements at a Glance
Validation and monitoring help keep AI safe after deployment. Drift shows up when what happens in production starts to differ from what you tested before launch. That’s why these controls matter so much: they connect initial approval to safe day-to-day use.
A governance framework should spell out three things clearly:
- how deep validation needs to go
- who owns each step
- when an issue needs to be escalated
The level of control should match the risk of the use case. Clinical AI needs the heaviest review. Administrative and documentation tools can use a lighter approach, but the rules still need to be clear and written down.
Use this snapshot to match validation depth to use-case risk.
| Requirement | Clinical AI (e.g., Sepsis Prediction) | Administrative AI (e.g., Revenue Cycle) | Documentation AI (e.g., Ambient Scribe) |
|---|---|---|---|
| Pre-Deployment Validation | 3-phase: Technical, Clinical, Deployment; multi-site testing [25] | Technical validation; ROI and accuracy stress testing [25] | Technical validation; PHI redaction accuracy; hallucination checks [25] |
| Post-Deployment Review | Shadow mode (2–4 weeks); clinical workflow integration audit [25] | Performance vs. baseline billing metrics; security audit [25] | Sampled human review; accuracy vs. clinical notes [25] |
| Continuous Monitoring | Real-time drift and calibration alerts; patient safety incident tracking [25] | Distribution drift; processing latency; error rate monitoring [25] | Hallucination rate monitoring; PHI leakage detection [25] |
| Subgroup Testing | High rigor: stratified by race, age, sex, and disease severity [25] | Moderate: insurance type and geographic disparities [25] | Moderate: accents, dialects, and terminology accuracy [25] |
| Escalation Triggers | Performance below threshold for 30 consecutive days; clinical safety event [25] | Significant drop in automation rate; security or access anomaly [25] | High hallucination frequency; PHI exposure incident [25] |
Before full activation, run shadow mode and compare the model’s outputs with actual outcomes. It’s a simple check, but it can catch problems before they hit live care or business workflows.
Clinicians should keep final decision-making authority and document overrides. Vendor terms also need to back up these controls, especially around training limits, logs, and notice when the model changes.
AI Incident Response Control Map
Building on the incident response roles already defined, this map shows how to respond by threat type. AI incidents don’t always fit a standard breach playbook. They can expose PHI, corrupt clinical output, and disrupt care. That’s why prompt injection, model tampering, poisoned training data, and unsafe outputs need threat-specific controls like rollback, provenance checks, output validation, and clinical review.
Section 6 defined who owns AI incidents. This map defines what each owner does.
| AI Threat | Immediate Containment | Owner | Logging Requirements | Escalation Path | Recovery Steps |
|---|---|---|---|---|---|
| Prompt Leakage / PHI Exposure | Disable the affected LLM or RAG endpoint; revoke API keys or service credentials; block unsafe prompts or malicious payloads [28] | CISO / Security Ops | Prompt and response logs; user and system context; timestamps; access logs | Security → Privacy/Compliance → Legal → Vendor Manager | Update guardrails; restrict PHI access; revalidate the endpoint before reactivation [28] |
| Model Compromise / Config Tampering | Roll back to a known-good model version; freeze configuration changes; isolate the endpoint | CISO / ML Ops / CIO | Model version IDs; config change history; access logs; deployment timestamps | Security → CIO → Clinical Leadership → Vendor Manager | Rebuild from trusted artifacts; verify model integrity; stage re-enablement with heightened monitoring [29] |
| Adversarial Manipulation (Prompt Injection) | Block unsafe prompts or malicious payloads; suspend the affected workflow; preserve payload and log evidence [31] | Security Ops / ML Ops | Anomalous prompt logs; output deviation alerts; token spike monitoring | Security → Clinical Leadership → Compliance → Legal | Add content filters; tighten retrieval restrictions; require human review for affected use cases [31] |
| Unsafe / Clinically Harmful Outputs | Suspend the AI-assisted workflow; switch clinicians to a manual fallback; flag affected cases [28][30] | Clinical Leadership / Patient Safety | Output logs; clinician override records; near-miss and adverse event reports | Clinical Leadership → Compliance → Affected Care Teams | Root-cause analysis; rollback to a validated version; updated human sign-off checkpoints [30] |
| Poisoned Training Data | Freeze training and fine-tuning jobs; isolate suspect data segments [29][32] | ML Ops / Data Science / Privacy | Training data provenance logs; performance anomaly alerts; intermediate output records | ML Ops → Security → Privacy/Compliance → Vendor Manager | Rebuild training sets from verified sources; retrain; validate against trusted benchmarks before reactivation [32] |
| Operational Disruption (AI Service Outage) | Activate pre-approved manual fallback workflows; isolate cascading dependencies | CIO / IT Operations | Service availability logs; dependency maps; incident timeline | IT Ops → CIO → Clinical Leadership → Vendor Manager | Staged service restoration; post-incident review of workflow resilience and vendor SLA compliance |
One point matters here: someone must have named authority to shut down an unsafe system. At the same time, logs need protection, and reactivation can’t be casual. It should require sign-off from security, clinical governance, and compliance, along with heightened monitoring after the system comes back online. [26][27]
This isn’t a hypothetical risk. Studies show prompt injection can lead to unsafe treatment advice and expose private data [28][31]. That means tabletop exercises shouldn’t stop at generic outage scenarios. They should include prompt injection, unsafe outputs, and vendor-side compromise.
Use these controls to update your risk register, revalidation triggers, and board reporting.
Conclusion
These seven conversations aren't one-and-done checklists. They're standing governance duties that need a regular place on the agenda.
Put them together, and they form one control chain: PHI protection, pre-deployment governance, clinical validation, vendor oversight, bias control, incident response, and enterprise risk alignment. In practice, that turns AI oversight into a repeatable operating model.
That model matters because the risk picture is getting tighter, not easier. Breaches still happen often, and OCR, the Joint Commission, CHAI, and FDA are tightening expectations for AI governance.[33][34][35][36][37][38]
Organizations that move now can deploy AI faster, with stronger safety and control. For healthcare AI leaders, the next step is straightforward: put these seven conversations on the standing risk agenda.
FAQs
How should we prioritize these seven risks first?
Use a structured, governed-by-design approach that builds security and compliance in from day one. Set up a cross-functional AI governance committee and a standard risk-management rubric to assess cybersecurity, clinical, and ethical threats.
Then sort AI systems by risk level, map sensitive data flows, and complete formal impact assessments before deployment. This spreads accountability across teams while helping manage patient safety, regulatory requirements, and shifting vendor risks.
What makes healthcare AI governance different from regular IT governance?
Healthcare AI governance is more than standard IT governance because AI can shape care decisions and, in turn, patient safety.
Standard IT governance usually centers on things like security and uptime. That matters, of course. But AI adds another layer of risk. A model can drift over time. An algorithm can show bias. And systems can face adversarial attacks that push them toward bad output.
That’s why healthcare AI needs oversight from more than just IT. It calls for input from clinical, legal, ethics, and data science teams. It also demands strict compliance, clear documentation, and clinical validation inside day-to-day healthcare workflows.
Who should own AI risk across the health system?
AI risk shouldn’t live in just one department. It works better when a multidisciplinary governance team shares it, so decisions reflect a mix of clinical, legal, technical, and security views.
Many health systems handle this through an AI governance board. These groups often include leaders from IT, cybersecurity, data privacy, compliance, and clinical teams. Clinical governance often takes the lead on model risk and patient safety, while the CISO is playing a bigger role in building security into the full AI lifecycle.
Related Blog Posts
- Healthcare AI Data Governance: Privacy, Security, and Vendor Management Best Practices
- Clinical Intelligence: Using AI to Improve Patient Care While Managing Risk
- The AI-Ready Organization: Cultural and Technical Prerequisites for Success
- The Future of Healthcare AI Will Be Governed or It Will Be Dangerous
