If I had to boil this article down to its core point, it’s this: healthcare teams need a clear AI governance process before AI touches PHI, clinical decisions, billing, or core systems. The webinar series focuses on five risk areas, shows what controls to put in place, and explains who should own each step from intake to audit records.
Here’s the short version:
- ECRI ranked weak AI governance as the No. 2 patient safety threat for 2025
- The series centers on 5 risk domains:
- patient data and cyber risk
- unsafe or biased outputs
- managing third-party AI risk
- governance gaps
- compliance exposure
- It walks teams through 3 main jobs:
- map PHI and AI data flows
- test outputs and set human review rules
- review vendors, assign owners, and keep audit records
- It uses the NIST AI RMF as the structure:
- Govern
- Map
- Measure
- Manage
- It recommends risk tiering before launch:
- low risk: periodic review
- moderate risk: drift, bias, and error tracking
- high risk: real-time monitoring, board approval, and clinical validation
What stands out is that the article does not treat AI as just an IT issue. I see it as a cross-team control problem. A bad AI output can affect care, claims, privacy, and system uptime at the same time. So the article pushes one clear answer: set one intake path, one ownership model, one inventory, and one record of review.
A few points matter most to me:
- PHI flow mapping comes first
- vendor contracts need AI-specific terms
- human review must be documented
- high-risk use cases need stricter checks before and after launch
Below that, the article explains how each webinar session turns those ideas into steps your team can use inside security, privacy, compliance, legal, IT, procurement, and clinical review.
From Deployment to Oversight: Strengthening AI Risk Management and Patient Safety in Health Care
sbb-itb-535baee
The 5 AI Risk Domains the Webinar Series Addresses
The webinar series groups AI risk into five areas where healthcare teams tend to face the most exposure.
| Risk Domain | Primary Impact | Common Control Gaps | Coverage Focus |
|---|---|---|---|
| Patient Data Exposure and Cyber Risk | PHI breach, EHR compromise, unauthorized data access | Insecure APIs, weak model access controls, unmonitored model-pipeline data exfiltration | Data flows and clinical integrations |
| Unsafe or Biased AI Outputs | Patient harm, clinician trust erosion, reimbursement denials | Automation bias, no clinical validation across subgroups, explainability gaps | Output validation and high-risk use cases |
| Vendor and Subprocessor Risk | Supply chain liability, shadow AI, PHI misuse by vendors | Missing AI inventories, opaque subcontractor data handling, no software bills of materials | Vendor assessment and contracting |
| AI Governance Gaps | Fragmented accountability, failed audits, uncoordinated response | No decision rights, inconsistent risk scoring, absent approval workflows | Ownership, intake, and approval workflows |
| AI Compliance Exposure | HIPAA/HITECH violations, FDA non-compliance, False Claims Act risk | No audit trail infrastructure, weak BAAs, undocumented human oversight | Audit readiness and regulatory documentation |
The next sections break down each domain in plain, practical terms.
Patient Data Exposure and AI-Driven Cyber Risk
AI systems create more ways for PHI to move, and that means more ways it can leak. A clinical summarization tool tied to an EHR, a chat-based intake system, or a document processing pipeline all open up new data flows that security teams have to map and watch.
Kiteworks points to five specific AI data breach risks in healthcare: inadequate training data access controls, insecure inference APIs, weak third-party protections, unmonitored model-pipeline data exfiltration, and retained model versions that still contain sensitive data.[1]
In practice, the trouble often starts with access that is too broad, least-privilege controls that aren't tight enough, and logging that leaves blind spots. Those issues can sit quietly in the background for months, then show up all at once when a breach forces everyone to look closer.
Unsafe or Biased AI Outputs in Clinical and Administrative Workflows
Risk climbs when staff lean too heavily on AI recommendations without stopping to question them. That kind of automation bias can show up in triage, coding, claims review, scheduling, and care navigation.[2][4]
Things get worse when a model performs unevenly across patient groups because the training data did not reflect them well. A tool may work well for one demographic group but post higher error rates for another. When that happens, existing health disparities can grow without much warning.[4]
There’s also a plain accountability problem. If a team can't explain why an AI system flagged a patient or suggested a code, it can't check the output with confidence, assign responsibility, or stand behind the decision during an audit. FDA guidance now says AI health tools should be built securely and should clearly spell out their limits and proper uses.[2]
Third-Party Vendor Risk, Governance Gaps, and Regulatory Exposure
Most healthcare organizations get AI through vendors or through tools with AI built in, instead of building the systems on their own. That shifts the risk rather than removing it. In many cases, it also makes the risk harder to track on paper.
A few questions matter right away:
- Does the vendor train external models on PHI?
- Who are the vendor’s subprocessors?
- What audit artifacts can the vendor provide?
HHS OCR is actively enforcing HIPAA against organizations that use AI without enough PHI safeguards, which turns governance gaps into an enforcement issue, not just a policy concern.[3] Health sector guidance now directly recommends banning vendors from using PHI or PII to train external models without prior written consent.[5]
Without a central AI inventory, clear decision rights, and updated Business Associate Agreements that deal with AI use in specific terms, organizations struggle to coordinate security, compliance, legal, clinical, procurement, and IT teams. Just as important, they struggle to show control when regulators come calling.
Governance gaps usually show up in simple ways: no clear owner for intake, no set approval path, and no steady monitoring. From there, regulatory exposure follows fast. If those gaps leave behind no audit trail, no record of human review, and no updated BAAs, the organization has very little to point to when questions start.
Together, these five risk areas frame the webinar’s guidance on controls, validation, and governance. The next sections show how the webinar translates those domains into control steps, validation checks, and ownership decisions.
Inside the Webinar Sessions: What Each Session Helps Teams Do
Each session is built around actions risk, compliance, and IT leaders can use right away. The content lines up with the risk areas covered earlier and moves in a clear order: risk domains, controls, validation, and ownership.
Securing AI Data Flows and Clinical Integrations
This session centers on one practical skill: knowing exactly where PHI moves in an AI-enabled setup and which controls apply at each step. Teams work through end-to-end PHI flow mapping, from ingestion to storage and logs.
The session turns zero-trust into concrete controls like least-privilege access, mutual TLS, and identity-aware proxies for AI APIs. Role-based access should keep licensed clinicians, administrators, and developers in separate lanes.
It also connects AI-specific threats such as data poisoning, prompt injection, and API abuse to the right controls. Recommended defenses include:
- API gateways
- Segmentation
- Provenance checks
Once teams have a handle on data flows, the series shifts to a different issue: whether the outputs are safe to use.
Validating AI Outputs and Managing High-Risk Use Cases
High-risk use cases need validation before deployment and after launch. Teams compare outputs against clinical guidelines, expert review, historical benchmarks, and fairness metrics.
Bias detection relies on stratified analysis by race, gender, age, and socioeconomic status. If teams find differential performance, the sessions lay out clear remediation triggers and restricted-usage criteria. Human oversight should set explicit escalation and review rules. The HHS nondiscrimination rule for patient care decision support tools took effect July 5, 2024, which shows why documented human oversight matters for compliance, not just good process.[6][7]
From there, the series moves into vendor review, accountability, and audit readiness.
Assessing Vendors, Defining Ownership, and Preparing for Audit
Vendor sessions give procurement, compliance, and security teams an AI-specific review checklist. The main questions focus on PHI use, subprocessors, and available audit artifacts. Teams also learn how to map fourth-party dependencies before signing a contract.
Governance sessions then help teams assign ownership with RACI-style responsibility matrices. These spell out who proposes, reviews, approves, and monitors each AI initiative. In practice, each use case should have one business or clinical owner, while security, IT, and compliance handle their parts. Every material model or integration change should trigger a documented review, along with logs covering:
- Access
- Data processed
- Outputs
- Overrides
Frameworks and Censinet Capabilities Featured in the Series
Applying the NIST AI Risk Management Framework in Healthcare
The webinar series uses the NIST AI Risk Management Framework (AI RMF) as the shared structure for healthcare AI governance.
In plain English, it gives hospitals one operating model for handling AI risk. Instead of treating each issue as a separate problem, the framework pulls the five risk domains discussed above into one control structure. It also adds AI-specific concerns like bias, robustness, and explainability. That means teams can look at data exposure, unsafe outputs, vendor risk, governance gaps, and compliance exposure through the same lens.
The webinar also shows how each function connects to day-to-day healthcare work.
The framework has four functions - Govern, Map, Measure, Manage. Together, they give hospitals a practical path from policy to day-to-day action. The table below shows how each function lines up with healthcare activities, the webinar topics tied to them, and where Censinet fits.
| NIST AI RMF Function | Healthcare Activity | Webinar Topic | Censinet Support |
|---|---|---|---|
| Govern | AI policy creation, risk appetite setting, board reporting, clinical leadership sign-off for high-risk AI | Policy | Censinet RiskOps™ centralizes policies, approval workflows, and governance documentation |
| Map | AI use case inventory, PHI data flow mapping, risk tiering, third-party dependency tracking | Vendor and data risk | Censinet RiskOps™ hosts AI asset records; Censinet AI™ summarizes vendor responses into structured risk profiles |
| Measure | Risk scoring, bias and performance evaluation across demographic groups, vendor security assessment, false-positive and false-negative monitoring | AI safety and vendor controls | Censinet RiskOps™ manages questionnaires and scoring; Censinet AI™ auto-completes assessments and generates draft risk summaries |
| Manage | Remediation planning, audit preparation, routing findings into existing cyber and compliance programs, monitoring model changes | Remediation and audit readiness | Censinet RiskOps™ orchestrates remediation tasks and dashboards; Censinet AI™ supports mitigation planning and review workflows |
For teams that are just getting started, the series recommends beginning with the Map function. That means building a simple AI registry for the clinical tools with the biggest impact and the systems that handle large amounts of PHI. It's a smart first move. You start with the tools that matter most, instead of trying to govern everything all at once.
Using Censinet RiskOps™ and Censinet AI™ for AI Risk Management
The series then shows how Censinet tools turn the framework into work teams can repeat without reinventing the wheel each time.
Censinet RiskOps™ acts as the main record for AI risk work. Policies, assessment questionnaires, findings, remediation tasks, and status dashboards all sit in one place. So instead of chasing version after version of spreadsheets, security, compliance, and IT teams work from the same source. Dashboards also surface board-level metrics, including high-risk systems, open remediation items, assessment status, and risk trends.
Censinet AI™ supports vendor risk review and human-reviewed automation across evidence validation, policy drafting, mitigation planning, and routing. It pulls out key vendor details such as encryption practices, data residency, access control models, subprocessor relationships, and data retention gaps, then routes gaps for review.
It can also compare vendor attestations against a hospital's AI security standards, flag gaps, and suggest mitigations like extra contract clauses or tighter logging requirements. For policy work, it can draft starter language for PHI handling, model lifecycle management, and bias monitoring. Legal and compliance teams then refine that language. Human reviewers still control every decision and sign-off.
The routing feature works a lot like triage in a hospital setting. Findings are sorted by severity and domain, then sent to the right owner - whether that's the CISO, privacy officer, or CMIO - along with suggested timelines.
These workflows set up the governance model covered in the next section.
Turning Webinar Insights Into an AI Governance Program
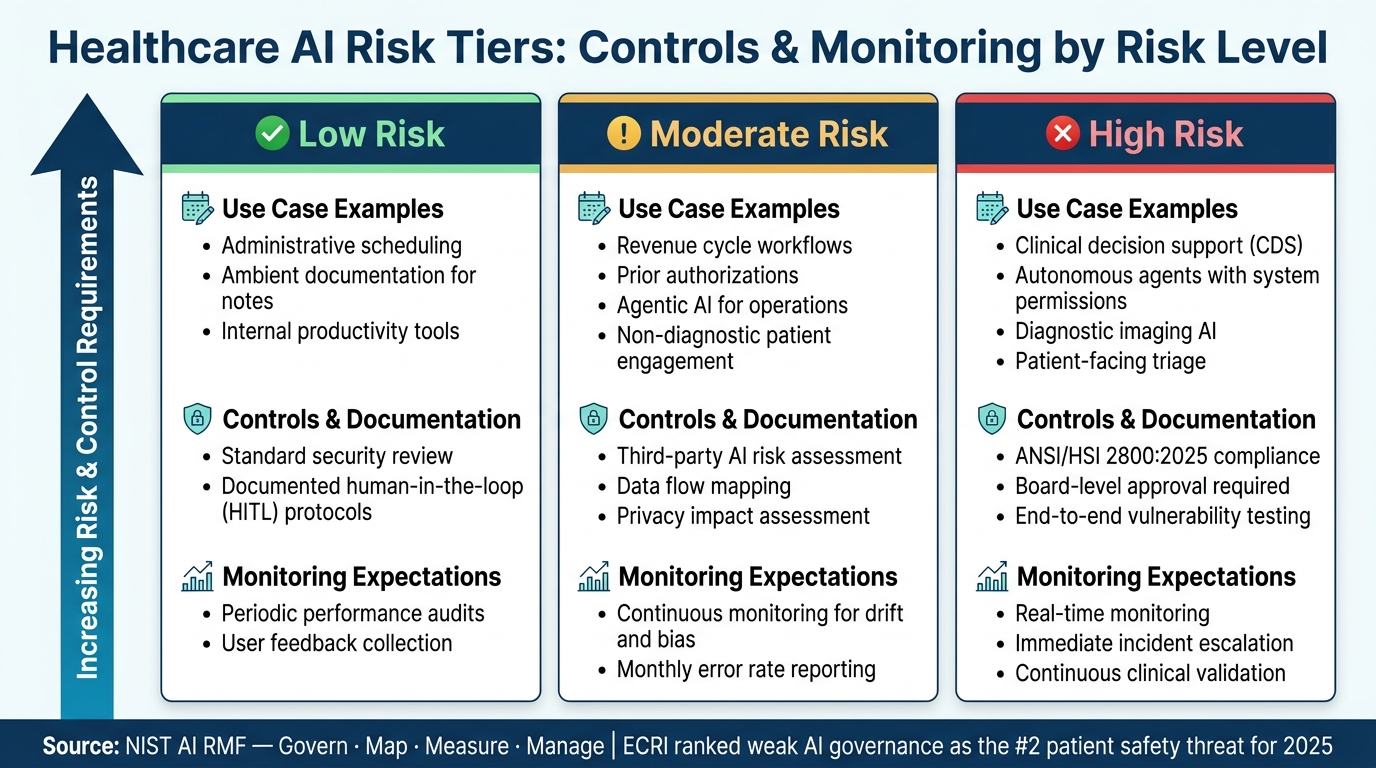
Healthcare AI Risk Tiers: Controls & Monitoring by Risk Level
Build a Cross-Functional AI Governance Model
The webinar advice becomes much more useful when you turn it into a repeatable governance process.
Start by assigning clear ownership for intake, approval, and monitoring for each AI use case. That sounds simple, but it matters a lot. If nobody owns a step, that step usually gets skipped.
Use the five risk domains as the basis for risk tiering and control selection. That gives teams a shared way to review AI use cases without inventing a new process each time.
AI governance also works best when it sits inside work people already do. Instead of running it as a side program, plug it into current security, privacy, compliance, legal, IT, and clinical workflows. That way, reviews feel like part of the job, not extra paperwork.
Procurement needs the same treatment. Build transparency and security checks into vendor review from the start, especially when outside tools will touch patient data, internal systems, or clinical workflows.
With ownership in place, the next move is to match controls to each risk tier.
Integrate AI Risk Into Existing Security, Compliance, and Monitoring Workflows
Fold AI risk into current security, compliance, and monitoring workflows. Before any AI use case goes live, classify it by risk tier. Then line up controls and monitoring with that tier.
Risk tiering turns governance into a repeatable review path.
| Risk Tier | Use Case Examples | Controls & Documentation | Monitoring Expectations |
|---|---|---|---|
| Low Risk | Administrative scheduling, ambient documentation for notes, internal productivity tools | Standard security review; documented human-in-the-loop (HITL) protocols | Periodic performance audits; user feedback |
| Moderate Risk | Revenue cycle workflows, prior authorizations, agentic AI for operations, non-diagnostic patient engagement | Third-party AI risk assessment; data flow mapping; privacy impact assessment | Continuous monitoring for drift and bias; monthly error rate reporting |
| High Risk | Clinical decision support (CDS), autonomous agents with system permissions, diagnostic imaging AI, patient-facing triage | ANSI/HSI 2800:2025 compliance; board-level approval; end-to-end vulnerability testing | Real-time monitoring; immediate incident escalation; continuous clinical validation |
Once use cases are tiered, monitoring, escalation, and documentation can follow the same playbook.
High-risk systems need real-time monitoring, immediate incident escalation, and continuous clinical validation. These are the tools most likely to affect care decisions, system access, or patient outcomes, so the bar has to be much higher.
Moderate-risk systems need continuous monitoring for drift and bias, along with monthly error rate reporting. This helps teams spot problems before they turn into workflow or patient-service issues.
Low-risk tools can lean on periodic audits and user feedback, but they still need documented approval and review. Even simple tools deserve a clear paper trail.
FAQs
How do we start AI governance in healthcare?
Start with a cross-functional committee that brings together clinical, IT, legal, and privacy teams. Then build an enterprise-wide AI inventory of the tools already in use across the organization.
A structured framework like PPTO helps you spot gaps before they turn into bigger problems. It also gives teams a clear way to review tools before they go live. That review should confirm:
- BAA coverage
- data residency
- audit trails
- risk tiers based on clinical impact
It also helps to line up oversight with emerging standards so executive leaders and the board have a clear view of accountability.
Which AI use cases are high risk?
In healthcare, high-risk AI use cases are the ones that can shape clinical decisions or directly affect patient outcomes. That’s why they need close oversight and careful review from regulators.
This group includes FDA-classified diagnostic tools, agentic AI systems that can act on their own with limited human oversight, and any tool that handles PHI without proper governance.
What should we ask AI vendors before approval?
Before approval, check the vendor’s entire supply chain. That means subcontractors, open-source dependencies, and whether the vendor can retrain models without telling you first. Use a standard framework, such as the HSCC guide, to review transparency and risk so the process stays consistent.
For any service that touches protected health information, require a BAA. You should also ask for AI transparency reports, alignment with NIST standards, SOC 2 audit reports, quarterly risk reporting, API audit rights, and breach notification terms that require notice within 24 hours.
