If your AI governance stops at policy, you have a gap. ANSI/HSI 2800:2025 is about turning board intent, executive ownership, vendor review, and clinical oversight into day-to-day actions that teams can prove.
Here’s the short version: I see this standard as a way to help healthcare groups move from “we have AI rules” to “we can show how those rules work in practice.” It covers the full AI lifecycle across clinical and admin use cases, ties work back to HIPAA, NIST, and HHS 405(d), and puts a big focus on third-party review, supply chain security challenges, evidence logs, and post-deployment monitoring.
If I had to boil the article down, these are the main points:
- AI governance needs named owners. The board sets direction. Executives put controls in place. Care and business teams apply them in daily work.
- One-time vendor review is not enough. Teams need repeatable steps for intake, approval, exceptions, reassessment, and fixes.
- Proof matters. Approval logs, consent records, audit trails, SBOMs, contract terms, and remediation records all help show that controls are active.
- High-risk AI should get more scrutiny. That includes tools tied to PHI, patient safety, clinical decisions, subcontractors, or core business functions.
- Third-party contracts need clear terms. Think breach SLAs, audit rights, vulnerability disclosure, PHI scope, and incident response duties.
- Post-launch review is a big part of the work. Models can drift, outputs can change, and new risks can show up after go-live.
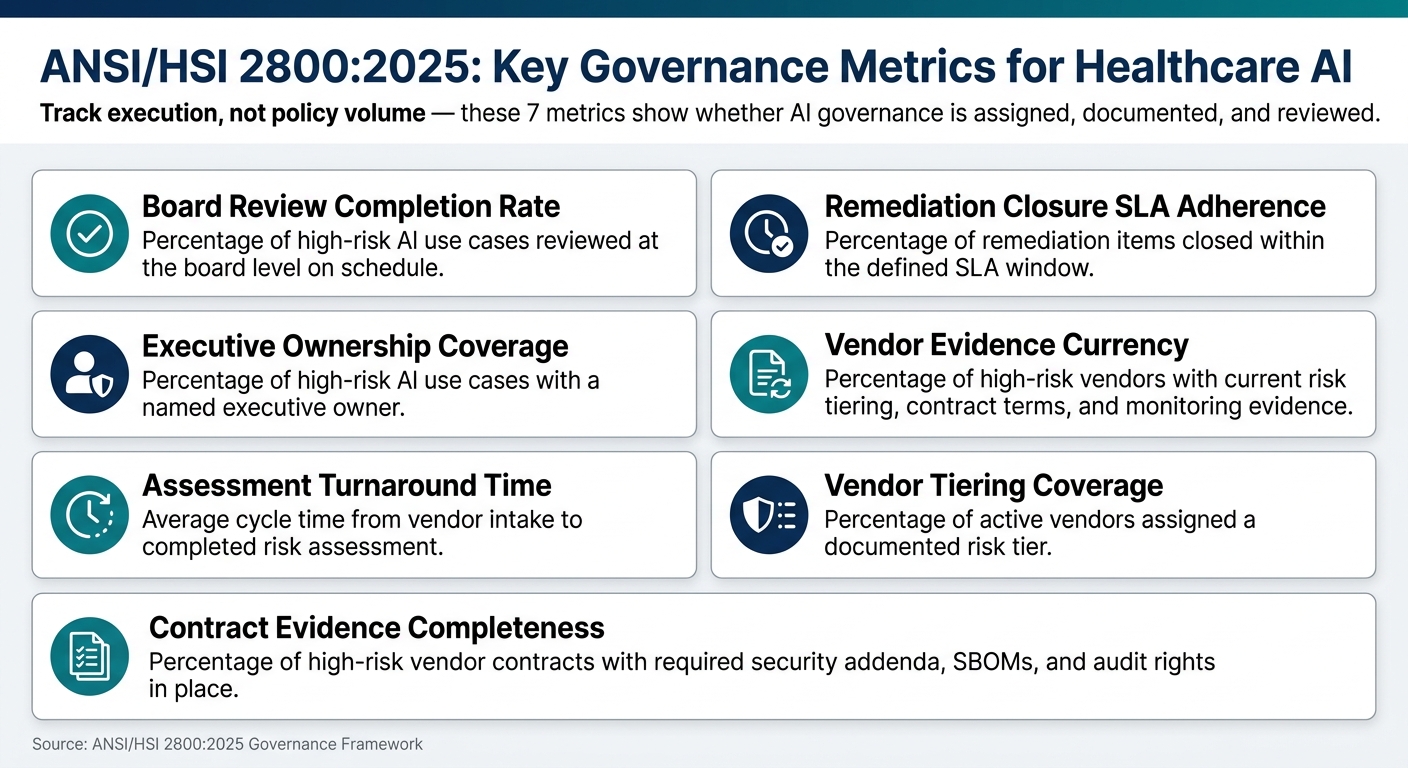
- Metrics should track execution, not policy volume. The article points to items like board review rate, ownership coverage, assessment cycle time, closure SLA performance, and vendor evidence currency.
A few details stand out. The article names seven core tracking areas for program performance, and it stresses that AI controls should cover both patient-facing and back-office tools. It also pushes teams to start where risk is often highest: third-party AI, supply chain review, and healthcare IT governance workflows.
So my takeaway is simple: ANSI/HSI 2800:2025 is less about writing new principles and more about making AI oversight visible, assigned, and repeatable. The rest of the article shows how to turn that into controls, records, vendor review steps, and board-level reporting.
Establishing an AI Governance Framework
sbb-itb-535baee
How ANSI/HSI 2800:2025 turns governance goals into controls
ANSI/HSI 2800:2025 turns governance goals into operational controls. In plain English, it moves teams from policy language to repeatable control execution.
Core governance structures and decision rights
One of the biggest shifts in the standard is that it treats AI oversight as an enterprise risk issue, not just a technical task. That means ownership has to stretch across teams. As HSI leaders note, boards and CEOs need a governance system that makes AI accountability real, and physician oversight is essential to review safety and outcomes. [1]
That kind of accountability can't rest on informal judgment or hallway conversations. Decision rights need documented workflows. Escalation paths should be written down for both clinical and operational AI use cases, so when a risk shows up, there’s a clear path to the right decision-maker.
Control mapping to HIPAA, NIST, HHS 405(d), and supply chain guidance
ANSI/HSI 2800:2025 does not replace HIPAA, NIST, HHS 405(d), or supply chain guidance. It adds more detail across the AI lifecycle:
- procurement
- development
- deployment
- monitoring
- continuous improvement
The point is to turn governance goals into day-to-day workflows. That includes patient consent, use disclosure, opt-out handling, bias mitigation, and safeguards against opaque tools. When those controls are spelled out and repeated the same way each time, teams can cut cyber, safety, and workflow risk.
The standard also calls for monitoring, auditing, and feedback loops after deployment. That matters because AI systems can drift, produce unintended consequences, or create safety issues over time. The same controls should apply to vendors and service providers too. So the standard becomes something teams can audit in daily operations, not just during launch.
Assessment tools and evidence artifacts the standard enables
Audit readiness under ANSI/HSI 2800:2025 depends on proof that controls stay active after deployment, not just on go-live day. Organizations should be able to show records such as approval logs, escalation decisions, monitoring logs, remediation and reassessment records, and consent and disclosure documentation.
Those artifacts create a clear chain from governance intent to operational execution. They show that controls are active, traceable, and open to review, which also helps with third-party reviews and supply chain monitoring.
Applying the standard to third-party risk and supply chain security
Third-party vendors, connected medical products, and AI services are some of the biggest risk points in healthcare. ANSI/HSI 2800:2025 sets a common approach for due diligence, contracting, and monitoring across the full vendor lifecycle. In practice, that starts with vendor tiering and due diligence.
Third-party AI due diligence and risk tiering
Not every vendor creates the same kind of risk. A scheduling tool is one thing. A predictive analytics system built into a clinical workflow is something else entirely.
ANSI/HSI 2800:2025 makes that difference clear by using inherent risk scoring based on factors such as PHI access, model purpose, hosting model, subcontractors, safety impact, and business criticality.
That scoring helps teams separate low-risk administrative tools from systems that can affect patient safety or care delivery. If a vendor's AI model has a direct role in clinical workflows or patient safety, the due diligence bar goes up.
Contract, evidence, and monitoring requirements
After risk tiering is done, the standard points to specific contract and evidence requirements. Business associate agreement terms need to match the actual scope of PHI use. Security addenda should spell out patch expectations and vulnerability disclosure practices. Breach notification SLAs, right-to-audit clauses, software bills of materials (SBOMs), and incident response participation requirements should all be written into the contract.
For example, an AI revenue-cycle vendor should provide an SBOM, disclose subcontractors, agree to incident-response participation, and accept a right-to-audit clause.
Those terms then shape the evidence and monitoring work that comes next. The standard calls for auditing and feedback loops to catch drift, unintended consequences, and new safety issues in AI-enabled services after deployment [1].
How Censinet supports standardized execution at scale
This is usually where spreadsheets and email chains start to fall apart. Managing these requirements across dozens or hundreds of vendors is hard to do by hand. Censinet RiskOps™ ties risk tiering, evidence collection, contracting requirements, and continuous monitoring into one workflow.
The table below maps vendor tasks to standard requirements and supporting workflows:
| Third-Party Risk Activity | ANSI/HSI 2800:2025 Requirement | Censinet-Enabled Workflow |
|---|---|---|
| Risk Tiering | Inherent risk scoring based on clinical and safety impact | Censinet RiskOps™: Automated tiering based on clinical and operational risk |
| AI Due Diligence | Review of dataset governance, model purpose, and PHI use | Censinet AI™: Faster questionnaire completion, evidence summarization, and downstream subcontractor risk capture |
| Evidence Collection | Centralized review of SBOMs, VDPs, and audit reports | Censinet Connect™: Streamlined evidence gathering from vendors |
| Contracting & SLAs | Enforcement of breach SLAs and security addenda | Censinet One™: On-demand risk management |
| Remediation Tracking | Collaborative workflows for closing security gaps | Censinet RiskOps™: Automated tracking and reporting of remediation progress |
Censinet AI™ speeds questionnaire completion and evidence summarization.
These vendor workflows feed approvals, exceptions, and remediation processes across healthcare IT governance.
Embedding ANSI/HSI 2800:2025 into healthcare IT governance and GRC workflows
These controls can’t sit in a separate binder or a side process. They need to fit into the GRC workflows teams already use every day.
ANSI/HSI 2800:2025 moves AI governance into the intake, review, approval, exception, and monitoring workflows healthcare teams already use [1].
Building repeatable workflows for approvals, exceptions, and remediation
Putting the standard into practice starts with clear escalation paths and repeatable review steps across the AI lifecycle [1]. Teams also need to collect the evidence that shows compliance: patient consent, privacy safeguards, AI-use disclosure, and bias mitigation [1]. Clinical staff and physicians should validate outputs before approval and during monitoring [1].
Once that structure is in place, the handoff into automated routing, approvals, and monitoring becomes much cleaner.
Using Censinet RiskOps™ and Censinet AI as a governance command layer
Censinet RiskOps™ brings policies, risks, findings, and tasks into one place. It includes automated assessments, Action Plans, role-based routing, and activity logs.
Censinet AI™ routes findings to named owners, supports required human review points, and shows real-time risk data in dashboards for boards and executives.
That traceability makes risk reduction and accountability measurable.
Measuring value and building an execution roadmap
ANSI/HSI 2800:2025 AI Governance Metrics Dashboard for Healthcare
Metrics that show risk reduction and accountability improvement
Once controls are in place, leaders need a small set of metrics that show the system is doing its job. The goal isn't to count policies. It's to track whether governance is documented, assigned, and reviewed at the board level.
Use operational measures, not policy labels, to track progress.
| Metric | What to Measure |
|---|---|
| Board review completion rate | Percentage of high-risk AI use cases reviewed at the board level on schedule |
| Executive ownership coverage | Percentage of high-risk AI use cases with a named executive owner |
| Assessment turnaround time | Average cycle time from vendor intake to completed risk assessment |
| Remediation closure SLA adherence | Percentage of remediation items closed within the defined SLA window |
| Vendor evidence currency | Percentage of high-risk vendors with current risk tiering, contract terms, and monitoring evidence |
| Vendor tiering coverage | Percentage of active vendors assigned a documented risk tier |
| Contract evidence completeness | Percentage of high-risk vendor contracts with required security addenda, SBOMs, and audit rights in place |
When you track these metrics over time, compliance, risk, and IT teams can show that governance is becoming more consistent and that ownership is clearer across the organization.
Key takeaways and first steps for adoption
Start with high-risk vendors. Map controls to current workflows. Assign board and executive owners. Then expand to the full AI inventory.
A practical place to begin is with third-party risk, supply chain security, and IT governance. From there, inventory AI use cases across patient care, revenue cycle, scheduling, and diagnostics. Next, map controls across procurement, deployment, monitoring, and continuous improvement. After that, prioritize high-risk vendors for tiering and evidence review, and assign board and executive ownership before expanding to operational teams.
Those early moves create the baseline needed to extend governance across the rest of the AI portfolio.
FAQs
Who should own AI governance in a healthcare organization?
Under ANSI/HSI 2800:2025, AI governance is treated as an enterprise risk. That means the Board of Directors oversees it, while the CEO and executive leadership are responsible for putting it into practice.
The standard also calls for clear, named accountability for each consequential AI system across its full lifecycle. In plain terms, every major system needs specific people tied to key decisions and approvals.
For example:
- A business sponsor approves the use case
- An independent validation lead handles sign-offs
- A business owner takes charge of production deployment
On top of that, the governance model should be coordinated by a senior executive who reports to the CEO.
How do we start applying ANSI/HSI 2800:2025 to third-party AI?
Treat third-party AI as enterprise risk from day one, not a once-a-year checklist item. That means using a continuous, evidence-based governance model with a formal intake process before deployment. The goal is simple: define impact, data use, and regulatory requirements early, before the tool is live and harder to control.
Vendors should also provide clear evidence, not just broad claims. Ask for materials such as an AIBOM, training data provenance, and bias and fairness testing. On top of that, require contractual transparency. That includes audit rights, quarterly risk reporting, and alignment with the same HSI certification standards used for internal AI.
What evidence should we keep to prove AI controls are working?
Keep an audit-ready, time-stamped record set for the full AI lifecycle.
That means keeping clear records from the moment a system is proposed through production use and later review. Include intake documentation that explains the purpose, data use, and risk tier. Keep executive approval on file before the system goes live. Save validation reports that cover bias and performance, along with incident logs, version history, and source-attribute logs.
For third-party tools, keep the contracts, standardized questionnaires, and records from continued monitoring. Taken together, these records should show who owns the system, how decisions are made in a repeatable way, and how the organization meets compliance needs.
