Most patient identity checks still ask for more data than they need. This article’s main point is simple: zero-knowledge proofs let a person prove a claim - like active insurance, portal access, or age - without handing over raw details like an SSN, full birthdate, or member ID.
I’d sum it up this way: if you want to cut PHI exposure, lower third-party risk, and better match HIPAA’s minimum necessary rule, ZKPs offer a different model. Instead of moving patient data from system to system, the patient’s device keeps the data local and sends only a cryptographic proof. That matters when over 80% of breaches involve stolen or weak credentials.
Here’s what the article covers at a glance:
- The problem: many healthcare identity flows still rely on reused personal identifiers
- What ZKPs do: prove a fact without showing the data behind it
- Where they fit: portal login, insurance checks, age checks, prescription pickup, and referral access
- How they work: prover, verifier, nonce, and proof rules like completeness, soundness, and zero-knowledge
- What deployment looks like: credential issuance, wallet storage, session handling, and revocation
- What to watch: replay attacks, linkability, biometric isolation, legacy EHR/IAM fit, and setup tradeoffs
A few details stand out:
- A portal can verify a registered patient without sending credentials to a remote server
- An eligibility check can confirm active coverage without exposing policy data
- An age check can prove someone is 18+ without sharing a full date of birth
- Some flows in the article cite about 78 ms proving time and about 140 ms verification
- zk-SNARKs use smaller proofs, while zk-STARKs avoid trusted setup but use much larger proofs
In short: I see this article as a guide to moving healthcare identity from “show me your data” to “prove your claim.” The cryptography matters, but so do policy, audit controls, and careful rollout. This transition is a critical component of managing broader enterprise risk across the organization.
NorthSec 2025 - Christian Paquin - Enhancing Identity Credential Privacy with Zero-Knowledge Proofs
sbb-itb-535baee
Core Concepts Healthcare Teams Need Before Implementation
Start with three concepts: roles, proof properties, and data flow.
Prover, Verifier, and Challenge-Response
In a patient portal login or an eligibility check, the prover is the patient’s device, usually a mobile wallet or app. It stores cryptographically signed credentials from a trusted issuer, like a hospital or government agency. The verifier is the system asking for confirmation, such as a telehealth portal, an EHR platform, or a payer. It uses a public key to check that the proof is valid without seeing the raw data underneath.
To stop replay attacks, where someone intercepts a valid proof and uses it again in a later session, the verifier sends a one-time nonce. That nonce is a one-use value the prover must include in a new proof, which shows the session is live and not a recycled exchange. That’s the piece that makes the interaction secure, not just mathematically clever. These roles sit at the center of every authentication flow that comes next.
Completeness, Soundness, and Zero-Knowledge
These three properties decide whether a ZKP system works in healthcare.
| Property | What It Guarantees | Why It Matters in Healthcare |
|---|---|---|
| Completeness | A legitimate patient with valid credentials will always be accepted | Patients aren’t locked out of their EHR or portal because of cryptographic failure |
| Soundness | An impostor cannot forge a valid proof | Unauthorized access to PHI is blocked at the protocol layer, not just by policy |
| Zero-Knowledge | The verifier learns nothing beyond whether the claim is true | No SSNs, birthdates, or identifiers are sent or stored during the interaction |
Together, these properties decide whether the system is ready for enrollment and login workflows in practice.
How ZKP Authentication Differs from Data Sharing
ZKPs prove identity claims. They do not transfer medical records. This guide focuses on identity claims and attributes, like enrollment status or age, not medical-record exchange.
The main difference comes down to where sensitive data lives. In a standard verification flow, PHI moves across the network and ends up in the verifier’s system. In a ZKP flow, sensitive identity data stays on the patient’s device, and only the cryptographic proof travels across the wire.
ZKP systems can also make separate authentications harder to connect to each other. That limits cross-visit profiling and cuts long-term privacy risk. These ideas lead straight into the enrollment and revocation flows in the next section. Implementing these flows requires a robust cybersecurity program for digital health innovators to ensure long-term compliance.
How to Implement Zero-Knowledge Proofs for Patient Identity
Implementation starts with three core choices: what to prove, how to issue credentials, and how to revoke them.
Step 1: Define Identity, Privacy, and Regulatory Requirements
Start by defining the smallest set of attributes each workflow needs, such as name, date of birth, patient ID, or member ID. The point is simple: verify identity claims without exposing more PHI than the workflow needs.
It also helps to separate routine linkability from audited traceability. For day-to-day interactions, use contextual unlinkability so patient activity can't be casually tied together across contexts. Then keep traceability for audited exceptions only.
Map each workflow to HIPAA's minimum necessary standard. In plain terms, the system shouldn't ask, "show me your data." It should ask, "prove your claim." That choice shapes both the credential format and the verification method.
For fraud investigations or malpractice cases, define a conditional traceability model at the start. In this model, identity-linkage duties are split between two independent authorities, so no single party can deanonymize a patient on its own. That only happens with coordinated authorization [1].
Step 2: Issue Cryptographic Credentials and Choose a Verification Model
Once those requirements are set, a trusted issuer can issue cryptographic credentials, such as verifiable credentials (VCs). After the claims are defined, choose the smallest credential set needed to prove them.
Those attributes are encoded into cryptographic credentials. Patients can then prove specific facts, like active enrollment or age eligibility, without handing over the raw data behind them. Signed credentials are stored in a patient-controlled digital wallet or inside the device's hardware-isolated Secure Enclave or Trusted Execution Environment (TEE).
The proof system should match the workflow. Here's a practical breakdown:
| Workflow | Recommended Model | Key Advantage | What the Verifier Receives |
|---|---|---|---|
| Patient portals / telehealth | zk-SNARKs | Proof size in hundreds of bytes; ~140 ms verification [2] | Cryptographic proof only |
| In-person registration | Multimodal ZKP (ZABA) | ~78 ms proving time; ~140 ms verification; high spoofing resistance [3] | Commitment vector |
| Eligibility / consent | CL-signatures | Selective attribute disclosure [1] | Specific claims only |
There is a clear tradeoff here. zk-SNARKs need a trusted setup ceremony. zk-STARKs avoid that step, but the proofs are much larger - tens of kilobytes instead of a few hundred bytes [2].
Step 3: Run Enrollment, Authentication, Session, and Revocation Flows
Once credentials are in place, the system needs four working flows: enrollment, authentication, session handling, and revocation.
- Enrollment: The device processes biometrics locally and stores only a non-reversible result. It registers a SHA-256 hash of the liveness check to stop duplicate enrollments without storing PHI [2][3].
- Authentication: The patient's wallet creates a fresh non-interactive ZKP, and the verifier checks it without receiving raw identity attributes.
- Session management: Use session-specific pseudonyms so the system can maintain continuity without creating a persistent identifier [1].
- Revocation: If a device is reported lost, the issuer removes the credential from the registry or distributed ledger. Lost credentials should be recovered through re-issuance, not security questions, so the same privacy protections stay in place [1][4].
Security, Compliance, and Deployment Tradeoffs
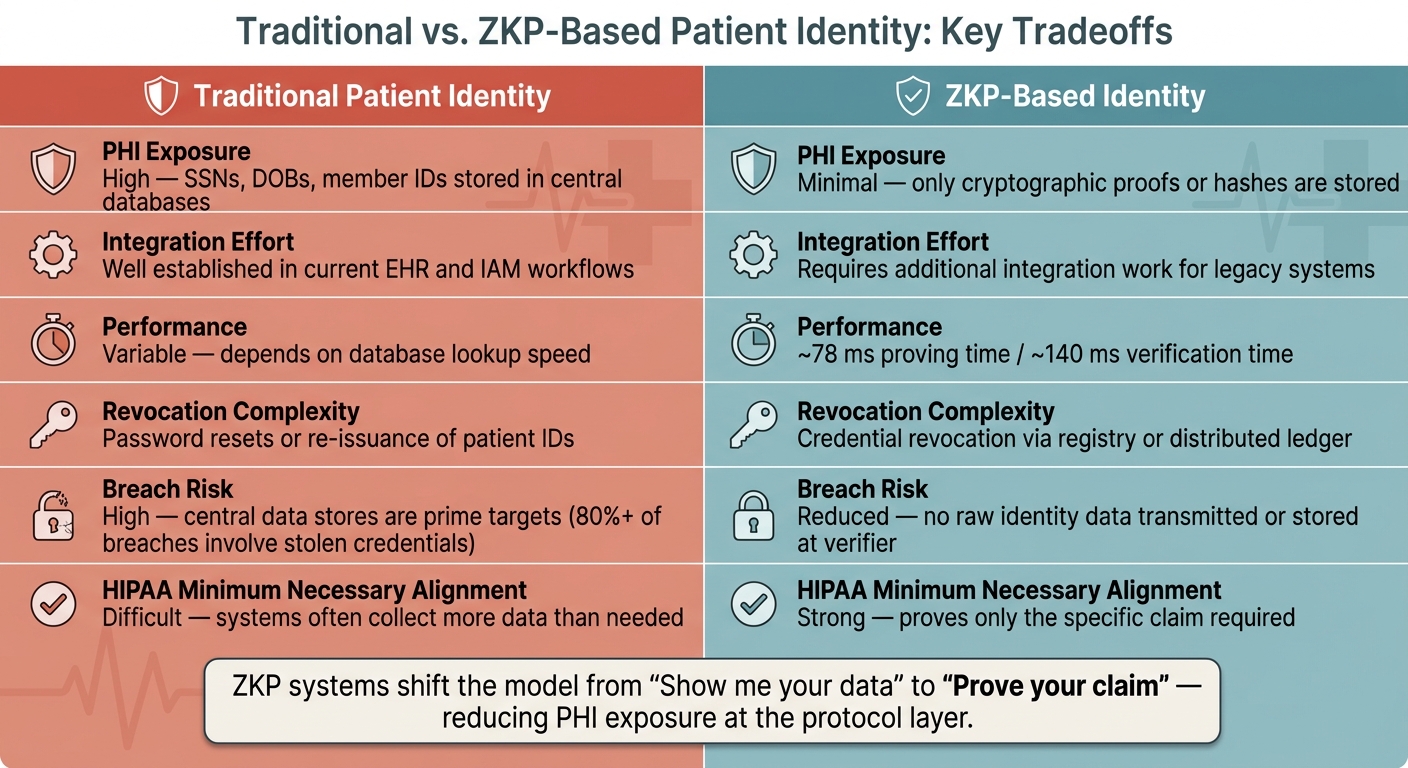
Traditional vs. ZKP-Based Patient Identity: Key Tradeoffs
Once the workflow is defined, the next step is to test it under attack, load, and audit pressure. This validation is critical for measuring what matters for cybersecurity in clinical environments. This is the last validation stage after enrollment, authentication, session handling, and revocation are already mapped out.
How ZKPs Reduce Identity and PHI Risk
The main security upside is straightforward: there's less sensitive data to steal.
Old-style identity systems collect and store sensitive identifiers like Social Security numbers, dates of birth, and insurance IDs in central systems. That makes them prime targets. ZKP systems cut that exposure down by storing only non-reversible hashes or cryptographic commitments.
Here’s the practical shift: a patient can prove active coverage without sending a policy number or member ID. The verifier gets only a proof, which means downstream systems never touch raw identity data.
What to Test Before Production Deployment
Don’t test only the clean, expected login flow. Test the protocol against the attacks people would actually try.
Before launch, security teams should check four things:
- Replay attack resistance: capture a valid proof and try to replay it in a later session.
- Unlinkability: even if a server is compromised, an attacker should not be able to connect an anonymous authentication session to a specific patient's real identity [3].
- Biometric isolation: for biometric-based setups, confirm that raw biometric data never leaves the device's Secure Enclave or TEE [2].
- Revocation: confirm that compromised credentials can be revoked and regenerated when needed [3].
That list sounds basic, but this is where weak deployments usually show cracks.
Implementation Pitfalls and Governance Requirements
After security testing, look at how the protocol fits with legacy EHR and IAM systems, as well as broader third-party risk management workflows.
The biggest day-to-day problem usually isn’t the cryptography. It’s integration. Many older EHR and IAM workflows were built to expect a patient identifier to be passed directly, so proof-based identity can force workflow changes. Teams should plan for that early, not halfway through deployment.
Cryptographic choices also carry governance risk. If you pick zk-SNARKs, you take on a trusted setup. If you pick zk-STARKs, you avoid that dependency, but the proofs are larger - often in the tens of kilobytes instead of a few hundred bytes [2]. Those aren’t just engineering choices. They affect risk posture, review scope, and audit conversations. Send those decisions through security, privacy, and compliance teams before production.
Benefits, Limits, and Rollout Considerations
ZKP-based identity verification can improve how patient identity is handled, but it also adds new moving parts. For U.S. healthcare teams weighing deployment, these are the tradeoffs that matter most:
| Dimension | Traditional Patient Identity | ZKP-Based Identity |
|---|---|---|
| PHI Exposure | High; sensitive data stored in central databases | Minimal; only proofs or hashes are stored [2] |
| Integration Effort | Well established in current workflows | Requires additional integration work for legacy systems |
| Performance | Variable; depends on database lookups | About 78 ms to prove and 140 ms to verify [3] |
| Revocation Complexity | Requires password resets or re-issuance of IDs | Involves revoking revocation records or credentials [3] |
A phased rollout makes the most sense. Start with patient-facing workflows, then move into tighter EHR-connected systems.
Conclusion: A Practical Path to Privacy-Preserving Patient Identity
After laying out the credentials, flows, and controls, the main takeaway is pretty simple: identity systems should reveal less. Many patient identity systems still pull sensitive data into a central place and then try to protect it with access controls. That approach can widen breach risk.
Zero-knowledge proofs change that setup. A patient can prove eligibility or a given attribute without sharing raw identifiers. The verifier sees only whether the proof is valid or invalid.
Putting this into practice comes down to a few plain steps: clear use-case scoping, careful credential design, tested authentication, and revocation. Compliance alone doesn't guarantee unlinkability or stop correlation across institutions.
The cryptography helps, but it can't carry the whole load. Policy has to spell out who can re-identify a patient, and under what conditions. In healthcare, governance matters just as much as the math. It needs to set the rules for when and how identity can be reconstructed.
For healthcare organizations looking at where privacy-preserving identity may fit, Censinet RiskOps™ supports risk assessments and benchmarking as teams review privacy-preserving identity in their security posture.
FAQs
Do zero-knowledge proofs replace patient portals and EHRs?
No. Zero-knowledge proofs don't replace patient portals or EHRs.
They add a privacy layer by confirming a patient's identity without exposing sensitive data. In plain English, they work alongside current systems rather than taking their place.
So the role is pretty simple:
- Patient portals and EHRs store, display, and manage health information
- Zero-knowledge proofs help verify identity with less data exposure
That means they complement existing systems, with a focus on tighter privacy and security.
What happens if a patient loses the device that stores their credentials?
If a patient loses the device that stores their credentials, they could lose access unless a backup or recovery option is already set up. Common options include social recovery or multi-party computation.
In most cases, the patient can contact the issuing healthcare organization to revoke the lost credentials and get new ones issued for a new device or another trusted recovery method.
How do healthcare teams choose between zk-SNARKs, zk-STARKs, and selective disclosure credentials?
Healthcare teams usually make this choice based on privacy, security, and performance.
zk-SNARKs work well for fast identity checks because they use short proofs and require little computation. zk-STARKs are a better fit when scalability and transparency matter more, since they don't need a trusted setup. And selective disclosure credentials let patients share only the data points that are needed, instead of handing over everything.
In practice, the decision is a balancing act between computational efficiency, trust assumptions, scalability, and the amount of privacy a given healthcare workflow calls for.
