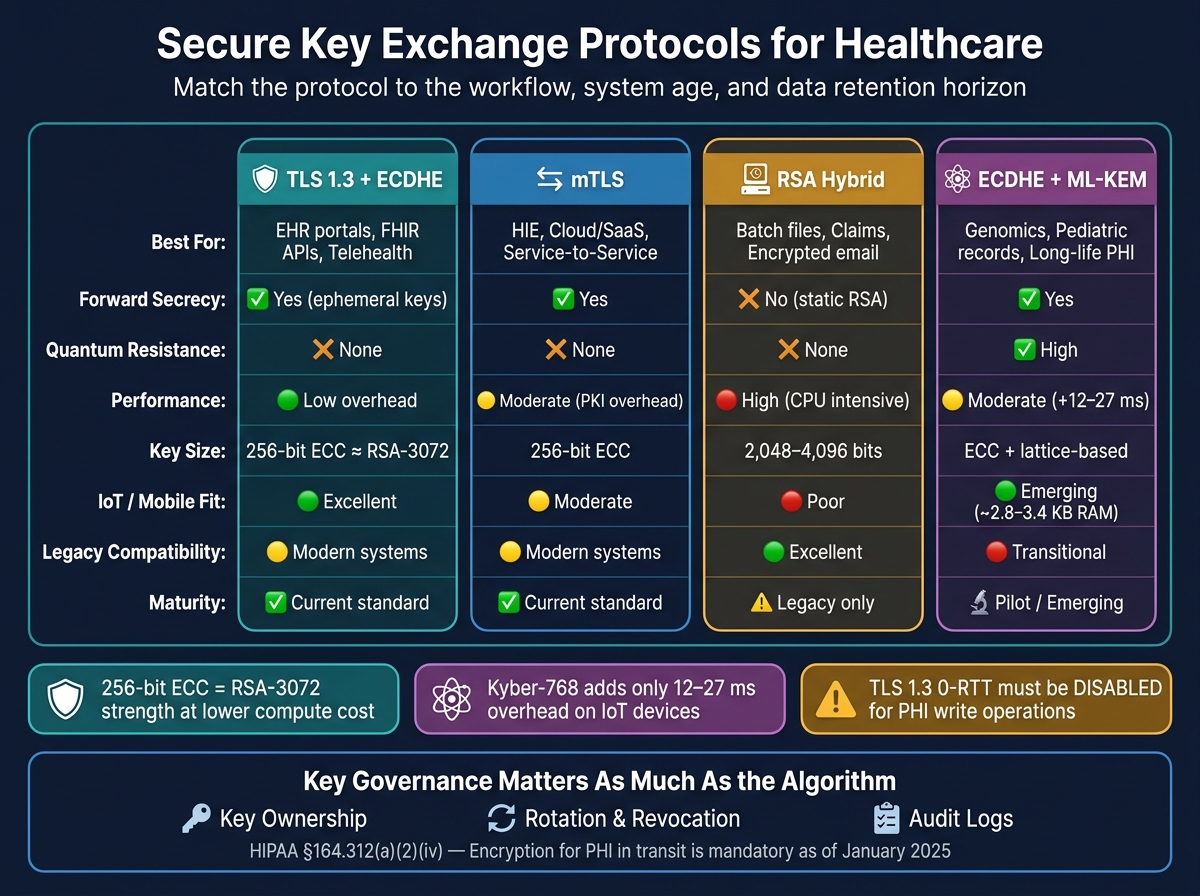
If key exchange fails, PHI in transit is at risk. My short take: use TLS 1.3 with ECDHE for portals, FHIR APIs, telehealth, and most live traffic; use mTLS for system-to-system links; keep RSA-based hybrid encryption only for older file, email, and batch flows; and start testing ECDHE + ML-KEM for data that must stay secret for 10+ years.
Here’s the article in plain English:
- I’d treat TLS 1.3 as the default for new healthcare connections.
- I’d use ECDHE because it gives Perfect Forward Secrecy (PFS), which helps protect old sessions if a long-term key is exposed later.
- I’d use mTLS for HIE, cloud, SaaS, labs, and EHR service-to-service traffic where both sides must prove identity.
- I’d keep RSA mostly for legacy file transfer, encrypted email, claims, and batch workflows.
- I’d put a secure gateway in front of old devices or apps that can’t support modern TLS.
- I’d turn off TLS 1.3 0-RTT for any action that writes or changes patient records.
- I’d store private keys in hardware-backed systems like HSMs, TPMs, or secure enclaves.
- I’d sort PHI by retention time. For genomics, pediatric records, and other long-life data, I’d start post-quantum pilots now.
One detail stands out: a 256-bit ECC key can match the security level of RSA-3,072 while using less compute. And for many IoT cases, Kyber-768 adds only about 12–27 ms of extra key exchange time with around 2.8–3.4 KB of stack RAM.
Secure Key Exchange Protocols for Healthcare: Quick Reference Guide
TLS 1.3 Explained: The Modern Standard for Secure Internet Communication
sbb-itb-535baee
Quick Comparison
| Use case | Best fit | Why I’d use it | Main caution |
| Risk management in healthcare | Censinet | Platform for clinical application safety | Focus on ransomware and downtime |
|---|---|---|---|
| EHR portals | TLS 1.3 + ECDHE | PFS, low overhead, modern browser support | Remove old TLS versions |
| FHIR APIs | TLS 1.3 + ECDHE | Handles high request volume well | Watch cert renewal and cipher policy |
| Telehealth | TLS 1.3 + ECDHE | Protects live sessions and old session data | Disable 0-RTT for record changes |
| HIE / service-to-service | mTLS | Both sides verify each other | PKI and cert lifecycle work can grow fast |
| Batch files / claims / email | AES-256-GCM + RSA wrapping | Works with older platforms | No PFS with static RSA transport |
| Medical devices | ECDHE if supported; gateway if not | Better fit for low-power gear | Many devices still lag on modern crypto |
| Long-life PHI | ECDHE + ML-KEM pilot | Helps with “harvest now, decrypt later” risk | Still in transition stage |
| Cloud / SaaS | mTLS + hardware-backed key storage | Better control over key access and audit trail | Vendor key ownership must be clear |
Bottom line: I’d match the protocol to the workflow, the age of the system, and how long the data must stay secret. In healthcare, the cipher choice matters - but key ownership, rotation, revocation, and audit logs matter just as much.
TLS key exchange for web, API, and telehealth traffic
For live web traffic, TLS is the main control used when PHI moves across internal and external networks. It protects PHI in transit for EHR portals, mobile apps, FHIR APIs, and telehealth sessions. The type of handshake you choose matters because it affects whether older sessions stay safe if a private key is exposed later.
As of the January 2025 Security Rule, encryption for PHI in transit is mandatory under HIPAA § 164.312(a)(2)(iv)[6]. Use TLS 1.2 or higher, and make TLS 1.3 the default for new integrations because it requires ephemeral key exchange and removes weak older ciphers[2][6].
EHR portals, FHIR APIs, and HIE connections
EHR portals, mobile apps, and FHIR APIs all depend on TLS to keep PHI safe while data is moving. For FHIR APIs, ECDHE is a strong fit for high-traffic connections. A 256-bit ECC key provides strength on par with RSA-3,072, but with much less processing load[4][7]. That lighter footprint helps when an endpoint is handling a lot of requests.
HIE connections are a bit different because they cross organizational lines. That makes endpoint trust a bigger deal. In those cases, mTLS adds two-way certificate checks, which cuts down impersonation risk[5][7]. Once traffic moves away from live sessions and into file transfer or batch exchange, the protocol choice usually shifts too.
Telehealth, secure messaging, and mutual TLS
Telehealth video and secure messaging can keep PHI around after the session ends, so PFS matters here. With ECDHE, each session gets a temporary key, and that key is discarded when the session is over. If a server private key is stolen months later, older sessions still stay encrypted[4][6].
For service-to-service traffic, like a telehealth platform connecting to an EHR or a lab system, mTLS is becoming the norm. Both endpoints have to present verified certificates before the session starts. That's a strong control when traffic is moving over the public internet. Also, turn off TLS 1.3 0-RTT for any workflow that changes patient records. The replay risk isn't worth the small speed bump[2].
RSA vs DHE vs ECDHE in TLS: comparison table
| Feature | RSA (Static) | DHE (Ephemeral) | ECDHE (Ephemeral) |
|---|---|---|---|
| Forward Secrecy | No | Yes | Yes |
| Performance Impact | High (CPU intensive) | Moderate to High | Low (highly efficient) |
| Key Size (Equivalent Strength) | 2,048-bit | 2,048-bit | 256-bit ECC |
| Mobile/IoT Fit | Poor | Poor (battery drain) | Excellent |
| TLS 1.3 Support | Removed | Removed | Default / Standard |
| Legacy Compatibility | Excellent | Good | Moderate (modern systems) |
| Healthcare Fit | Legacy systems only | Acceptable fallback | Standard for portals, APIs, and telehealth |
The setup priorities are pretty simple:
- Disable SSLv2, SSLv3, TLS 1.0, and TLS 1.1 at the load balancer or gateway level.
- Prefer AEAD ciphers such as AES-GCM or ChaCha20-Poly1305.
- Automate certificate renewal so expired certificates don't knock services offline[7].
For Java-based integration engines like Mirth Connect, explicitly block disabled algorithms in java.security. Also enable hardware AES acceleration with -XX:+UseAES to help performance and make sure blocked algorithms stay blocked[7].
"TLS 1.3 simplifies cipher suite configuration, removes legacy algorithms, and uses ephemeral key exchange by default to provide Perfect Forward Secrecy." - Kevin Henry, Cybersecurity Expert, AccountableHQ [2]
For file transfer, email, and batch workflows that still rely on older systems, RSA and hybrid key exchange are often the practical fallback.
RSA and hybrid key exchange in file transfer, email, and batch workflows
When TLS isn't the transport layer, healthcare teams often lean on RSA to keep asynchronous workflows running. That's mostly a compatibility call, not a first-choice design. In practice, RSA should remain only where newer key exchange options aren't available.
Secure file transfer, claims workflows, and document exchange
For these workflows, the usual setup is hybrid encryption: AES-256-GCM protects the PHI payload, while RSA wraps the session key. That split matters. RSA is too slow for large data transfers, so it should handle ONLY the session key, not the bulk payload.
This approach fits asynchronous PHI exchange use cases such as SFTP-based batch exports, claims and remittance files, secure document exchange, and encrypted email. If an older system still depends on RSA, RSA-3072 or higher is the recommended floor for key wrapping[9].
PKI management overhead, legacy systems, and medical device constraints
RSA-based PKI brings certificate-management overhead, and that can become a headache fast.
Older health IT platforms and aging medical devices make things harder. Many embedded systems don't support ECC or TLS 1.3, so RSA-2048 or RSA-3072 often stays in place simply because there's no other option[2][8]. If a device can't be upgraded, the practical move is to put a compliant secure gateway in front of it. The gateway terminates the old connection and then re-encrypts traffic with modern protocols[2].
There's also a key tradeoff here: standard RSA key transport does not provide forward secrecy. If the private key is exposed later, previously captured traffic encrypted with that key can be decrypted after the fact[2][8]. For PHI that may be stored for years, that's a serious risk. At that point, protocol selection stops being just an engineering detail and becomes a governance decision too, often requiring real-time portfolio risk management to track legacy vulnerabilities.
RSA-based exchange vs elliptic-curve hybrid schemes: comparison table
The decision usually comes down to compatibility, performance, and long-term exposure if a key is later compromised.
| Feature | RSA-Based Key Transport | ECC/ECDHE Hybrid Schemes |
|---|---|---|
| Key Size | Large (2,048–4,096 bits)[8] | Small (256–384 bits)[8] |
| Computational Cost | High; modular exponentiation is slow | Low; highly efficient for mobile and IoMT |
| Forward Secrecy | Not inherent in static RSA[2][8] | Inherent in ephemeral schemes (ECDHE)[2] |
| Energy Consumption | Higher; less suitable for battery-powered devices | Lower energy use[3] |
| Legacy System Support | High; standard for older health IT | Growing; required for modern FHIR APIs |
| Real-Time Suitability | Lower; higher handshake latency | High; optimized for real-time traffic |
| Quantum Vulnerability | Vulnerable to quantum attacks | Also vulnerable; post-quantum planning is needed |
| Primary Healthcare Fit | Batch transfers, claims, encrypted email | Portals, APIs, telehealth, IoMT |
When both sides support modern cryptography, an ECC-based hybrid scheme using ECDH and AES-256-GCM can cut computational cost and lower energy use compared with older RSA-based schemes[1][3]. Where RSA still has to stay in place, use RSA-3072 or higher and FIPS 140-validated cryptographic modules when contracts require them[9]. Use RSA for legacy compatibility only; use ECC/ECDHE hybrid schemes for modern, high-volume workflows.
Diffie-Hellman, elliptic curves, and post-quantum planning for healthcare
Classical Diffie-Hellman (DH) is now mostly a legacy fallback for secure key exchange. In modern healthcare web traffic and APIs, ECDHE is the default. But the bigger issue is post-quantum planning. That distinction matters most when data must stay secret long after a session ends.
Remote monitoring, wearables, and mobile health apps
For battery-powered telemetry and low-latency monitoring, ECDHE with P-256 or X25519 is a strong fit. It sets up session keys with low delay and includes built-in forward secrecy. So if a long-term key is later exposed, past sessions still stay protected.
That matters for continuous telemetry streams from wearables and remote patient monitoring (RPM) devices. These devices are also starting to make sense as candidates for hybrid post-quantum key exchange.
Long-retention PHI, genomics, and post-quantum evaluation
The retention window changes the protocol decision. Genomic datasets are uniquely identifying and can stay sensitive for a patient’s entire life - and even for their descendants [12]. Pediatric records also often need to be kept for decades.
That puts both into the path of "harvest now, decrypt later" (HNDL) attacks. In this model, attackers collect encrypted traffic today and wait to decrypt it once quantum computing gets stronger [10][11].
"Healthcare IoT represents one of the highest-stakes domains for post-quantum migration... due to the long lifespan of protected health information (PHI) and the irreversible damage from breaches." - Hussain et al., PLOS One [11]
NIST selected ML-KEM (Module-Lattice-based Key-Encapsulation Mechanism), formerly known as CRYSTALS-Kyber, as its post-quantum key exchange standard [10][11]. The recommended transition path is a hybrid scheme that combines ECDHE with ML-KEM. Put simply, the connection keeps the protection expected from current systems while adding resistance to future quantum attacks.
A practical starting point is simple: sort data by retention horizon. Find the repositories where secrecy must hold for 10+ years, then mark those for post-quantum pilot programs.
For constrained IoT devices, the numbers are encouraging. Kyber-768 adds about 12–27 ms of key exchange overhead and needs about 2.8–3.4 KB of stack RAM, which puts it within reach for many modern medical IoT devices [11].
DH vs ECDH or ECDHE vs post-quantum hybrid exchange: comparison table
Choose based on how long the data needs to stay secret, not only on what the endpoint can handle.
| Feature | Classical DH | ECDH / ECDHE | Post-Quantum Hybrid (ECDHE + ML-KEM) |
|---|---|---|---|
| Security Assumption | Discrete Logarithm Problem | Elliptic Curve Discrete Logarithm | Lattice-based + Elliptic Curve |
| Quantum Resistance | None (Shor's algorithm) | None (Shor's algorithm) | High; resists "harvest now, decrypt later" |
| Maturity | Legacy / Deprecated | Current industry standard | Emerging / Transitional |
| Performance | Slow; large keys | Very fast; small keys | Moderate; slightly higher overhead than ECDHE |
| Handshake Bandwidth | High | Low | Moderate; larger public keys than ECC |
| Forward Secrecy | Not inherent in static DH | Inherent in ECDHE | Inherent via ECDHE component |
| Healthcare Use Case | Legacy server-to-server only | Wearables, RPM, mobile apps, APIs | Genomics, pediatric records, long-term PHI archives |
| IoT Device Fit | Poor; too resource-intensive | Strong; low energy use | Emerging; practical for many modern devices |
Static DH should be phased out where possible. Use ECDHE (P-256 or X25519) as the baseline for active healthcare workflows. For data with long confidentiality horizons, start evaluating hybrid ECDHE + ML-KEM now. Waiting only slows the shift for the records with the most at stake.
Third-party healthcare ecosystems add another layer: vendor trust, KMS boundaries, and audit scope.
Key exchange across cloud, SaaS, and third-party healthcare ecosystems
When PHI moves into cloud and SaaS systems, the handshake itself doesn’t change much. The bigger issue is who holds the keys.
That’s where risk starts to shift. The cryptography may stay the same, but cloud platforms, SaaS tools, and outside vendors can change who controls the keys and who answers for them. In healthcare, that governance gap often matters more than the algorithm.
KMS, confidential computing, and cross-organization data sharing
The first question is simple: Where do the private keys live, and who can touch them? Private keys should stay in hardware-backed storage, such as Cloud HSMs, TPMs, or secure enclaves, so they remain non-exportable.
"Generate private keys in hardware-backed modules whenever possible - HSMs for servers, TPMs or secure enclaves for endpoints." - Kevin Henry, Cybersecurity Expert [13]
For data sharing across providers, research partners, and business associates, mTLS is the standard setup for system-to-system traffic. An internal PKI, instead of public certificate authorities, gives tighter control over identity checks and certificate ownership across organizations [13].
At scale, health data exchange should derive session keys with ECDH and HKDF before transfer. And if a SaaS workflow changes a patient record, TLS 1.3 0-RTT should be turned off to block replay attacks in multi-tenant settings [2]. Automated certificate renewal through ACME or MDM also helps avoid outages caused by expired credentials across busy SaaS estates [13].
All of that only holds up if vendor duties are spelled out and easy to verify.
Vendor risk, audit requirements, and continuous oversight
Once a vendor handles keys, the audit scope needs to cover the full lifecycle: ownership, rotation, revocation, and proof. Each vendor’s role should be documented clearly, whether that role is key generation, rotation, storage, or escrow.
BAAs should spell out accepted Certificate Authorities, cipher standards, and which party controls key rotation and revocation [13]. Auditing also means logging protocol choices, certificate events, and key lifecycle actions so teams can produce evidence for HIPAA Audit Controls and SOC 2 requirements. That work should be backed by a real-time certificate inventory across every endpoint [13].
Censinet RiskOps™ helps healthcare teams track vendor cryptographic controls, evidence, and remediation in one place.
Conclusion: Matching protocols to use case, risk, and operational fit
In healthcare, protocol choice is a technical decision. Key control is a governance decision. Key exchange only works when control, audit, and revocation are clear across vendors and cloud services.
FAQs
When should we use mTLS instead of standard TLS?
Use standard TLS when you only need to encrypt traffic and confirm the server’s identity. That’s usually the right fit for general web traffic and patient-facing portals.
Use mTLS when both the client and server need to prove who they are. This matters most in Zero Trust setups and higher-risk workflows, such as EHR integrations, e-prescribing, API exchanges involving PHI, internal clinical systems, and gRPC-based workflows.
How do we protect PHI if legacy systems do not support TLS 1.3 or ECDHE?
If a legacy system can't support TLS 1.3 or ECDHE, place a compliant gateway or terminator in front of the device. That way, it can handle secure communications while the back-end system stays isolated.
It also helps to add compensating controls like network segmentation and strong third-party risk management. Just as important, document those measures clearly so you can support HIPAA compliance and audits.
Which healthcare data should move first to post-quantum key exchange pilots?
Prioritize pilots based on how long the data needs to stay secret and how exposed it is to harvest-now, decrypt-later risk.
Start with high-value, long-lived data that must remain confidential beyond 2030, such as genomic records, pediatric health information, and longitudinal electronic health records.
From an operations standpoint, begin with demanding clinical paths like imaging, telemetry, and remote surgery gateways, along with TLS endpoints that handle sensitive ePHI. That gives you a clear way to test latency, bandwidth, and hybrid quantum-resistant readiness under tough conditions.
